
Mystery Disease: Tests for Whooping Cough Are Expensive and Slow


Certainty: That I am being treated for the right condition. That the drugs I’m taking aren’t going to be worse for me than the disease. That the horrible cough I had – so violent it felt like it would end me – is something I can avoid in the future.
It's not always possible as Deborah Kotz described in a 2009 piece for USA Today:
Doctors are stumped by symptoms all the time, and by prescribing the wrong medication, they often worsen the problem or even create a new one. Worse, misdiagnoses lead to an astounding 40,000 to 80,000 hospital deaths every year, according to a March paper published in the Journal of the American Medical Association—plus an uncounted number due to mistakes in the doctor's office. In fact, some 5 percent of autopsies find a condition missed by doctors that, if treated, might have saved the patient's life.
I wanted certainty, and I thought that getting tested for whooping cough would have provided me some.
But first I had to wait. My doctor told me the test results would take a week. That should have given me some certainty by July 19. I called the clinic, but the results weren’t in yet.
“It can take 10 working days after we send in the cultures, and we didn’t send them in until July 15. That should mean July 30.”
I called on the 30th. This time I was told there is typically a 12-day turnaround.
But I also was told something even more interesting:
“Pertussis is a fairly expensive test to run, so they hold the cultures until they have a batch of them and only run them once a week. They have to justify running the machine. The lab doesn’t even do them itself. They ship them to an outside source. The equipment is very expensive to buy and maintain.”
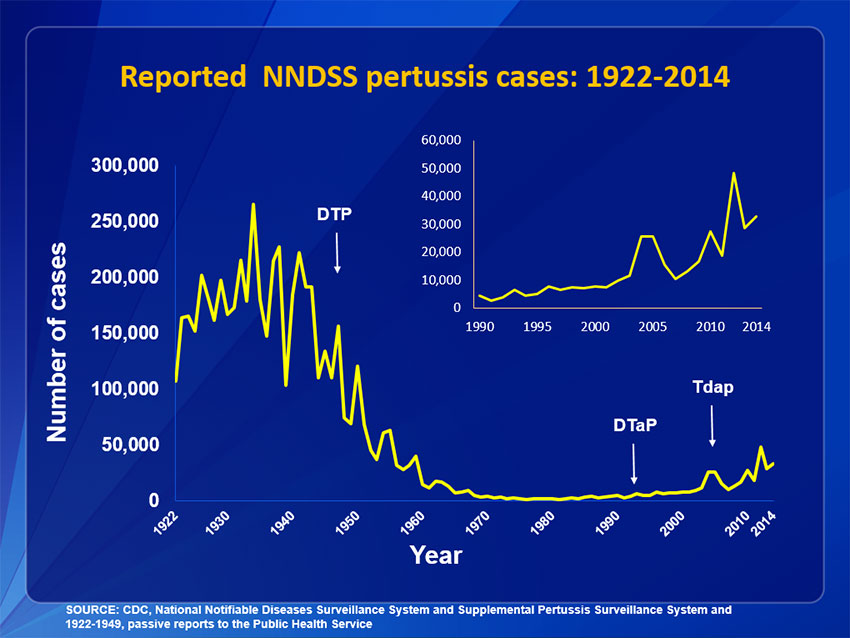
This seemed troubling. We are in the middle of a whooping cough resurgence. The first vaccination efforts drove the number of whooping cough cases down from a high of more than 250,000 nationwide in the 1930s to under 5,000 in 1990. New vaccination formulations in the mid-1990s and then the mid-2000s followed. But so did a rise in cases. In 2012, the number was climbing past 40,000 for the first time in more than 50 years. A commentary in the New England Journal of Medicine in 2012 called the resurgence an epidemic.
{kind=link}
The rise in cases is so alarming that state and federal public health agencies are constantly on the look out for new cases and deaths. The CDC reports the latest numbers weekly. As of the most recent report, there had been 11,799 cases in the U.S. this year.
But state and federal agencies rely on doctors offices and laboratories to report positive test results and deaths from the disease. How can new cases be accurately captured if labs delay running the tests for weeks because they are too expensive to run?
I also wondered about whether the tests would be less effective the longer the specimen sat around. “They keep the sample refrigerated,” I was told. “When you’re talking about a virus, it’s all dependent on what the specimen is, and some have shelf lives for quite a period of time. The lab wouldn’t have a 12-day turnaround time if the specimen was not viable.”
Pertussis is caused by bacteria, not a virus. But I didn’t want to quibble. I just wanted my test results.
So I called again on what would have been the 12thday. When the test results were still not in. I asked if I could call the lab directly. Here’s what the lab at Northwest Hospital, where my specimen was sent, told me:
“The tests can take up to 15 days.”
So I asked whether this would put young children jeopardy. The disease is particularly fatal in kids, and it would seem that not knowing for 15 days whether there was a pertussis outbreak in, let’s say, a kindergarten class would be a huge problem.
“Oh no,” the woman in the lab told me. “If you were a child, they would have run your test already. They run the tests for children always before adults, and so you’re probably getting bumped back by tests for children.”
I decided to just stop calling and to stop worrying. I felt better. Either the drugs worked, or my health improved on its own.
On Aug. 3, I received a letter in the mail from my doctor’s office. A full 22 days after I went in for an evaluation, the results on my test for whooping cough were in. And they were negative.
So what did I have? I probably will never know. But it is worth noting that the tests for pertussis have their own problems. As the CDC reports:
Culture is best done from nasopharyngeal (NP) specimens collected during the first 2 weeks of cough when viable bacteria are still present in the nasopharynx. After the first 2 weeks, sensitivity is decreased and the risk of false-negatives increases rapidly.
By the time I saw a doctor, I had been coughing for more than two weeks, so I was in the decreased sensitivity window when she took my sample. The upshot? My negative test could be false. There’s no way to go back in time and get a better, earlier sample.
It’s been a lesson for me that often certainty is unattainable in medical care. It’s something my friends who are physicians and scientists live and breathe every day, but patients expect certainty from science.
With improvements in testing protocols; with better physician education about signs and symptoms; with more rapid and widespread reporting of the disease, we may get closer to certainty with whooping cough.
For now, I’m going to have to take it on faith that I had something nasty and – perhaps with the help of medicine – beat it. That’s a small victory. And I’m grateful for it.
Image by Amy Loves Yah via Flickr