
Learning to respect a patient's wishes at the end of life
The nation spends billions of dollars on care like this for patients during the last year of life. And a recent Institute of Medicine report found all that spending isn’t necessarily helping us live longer or better. Is there a better way to help patients nearing the end of their lives avoid the kind of care they don't want and get the care they prefer - whether it's staying home, easing pain, or aggressive treatment? There's an experiment underway to find out.

Talking about dying is difficult for most people, including doctors. But can they learn a better way to help patients nearing the end of their lives? Can health care systems learn to respect those wishes? Here’s one experiment to find out.
Doctor Kate Lally gathers a group of second year residents outside a patient’s room at Kent Hospital in Warwick, Rhode Island. Lally explains the patient they’re about to examine is 34 year old Melissa Smith. She has advanced ovarian cancer. Until now, she’s been in hospice care at home, keeping comfortable.
“While home on hospice, she develops severe pain. She comes to the emergency room, looks like she’s got a bowel obstruction,” Lally explained.
Lally is head of palliative care for Care New England hospitals. That’s a relatively new specialty for the hospital system, one that’s focused on alleviating symptoms and easing pain in patients with a terminal illness.
Lally pulls back the curtain and sends in the first resident, Doctor Desirae Budi, to figure out what to do next. Patient Melissa Smith stiffens and pants in her hospital bed. Her mother grips her daughter’s hand.
“Hi Mrs. Smith. I’m Doctor Budi here. Can you tell me what’s going on?”
Budi can see Smith needs something stronger for the pain. She tells the mother she’ll be back with a plan. Behind the curtain, she debriefs with Lally about some options – maybe switch the morphine out for another medication, maybe give Smith something to relieve the anxiety? Clearly, she’s dying, Budi says.
Happily, this is just a simulation. Melissa Smith is actually Melissa Bowler, an actress. Doctor Kate Lally is using this simulation to teach residents how to talk to patients and their families about dying…and how to listen to what they want in their final months, days, or hours. Next up is second year resident Doctor John Sullivan. Lally tells him two hours have passed. Now Smith is delirious, unresponsive. She seems to be picking at the air, trying to grab something unseen. Her mother wants some reassurance about what’s happening.
Sullivan: “As far as how long this process may take…”
Smith’s Mother: “What process? I think she’s dying.”
Sullivan: “She very well…. It very well could be.”
Each resident tries hard to help. But this is clearly uncomfortable for everyone in the room. When the simulation ends, Lally offers some feedback. It’s OK, she tells the residents, to tell families a patient is dying. They want to know what to expect.
“I’ll often use wish statements…I’ll say things like, I wish you weren’t going through this. I’m so sorry this is happening. I wish this wasn’t happening. What we can do at this point is make sure she doesn’t suffer…”
Back in her office at Kent Hospital, Doctor Kate Lally says the training is part of a larger movement called The Conversation Project. Her employer, Care New England, is one of 10 health care systems around the country trying to become what’s called “conversation ready,” pioneering ways to put patient wishes first and keep a record of those wishes. Lally says that’s what doctors should be doing automatically. But it doesn’t always happen that way.
“And often if you just ask people what they want they’ll tell you. And very often we just didn’t ask.”
Lally is betting that doctors can be taught to ask, and to listen better. They might not be as familiar with what to do with that information. So Lally created a new position called a Conversation Nurse – she’s hired two so far, and she’s looking for a third. Conversation nurses are on call for doctors who want some help navigating those end-of-life decisions with patients. Lally says word is getting out about the service.
“From august of 2012 to the end of the year we had about 65 consults. … And then last year for 2014 we had 997 requests for consult.”
Lally says the service costs the hospital system a little money, but it could save money in the long run – even though that’s not the primary goal.
“I always say I don’t promote this kind of care because it’s less expensive. I promote this kind of care because it’s better. A patient being with their family at home when that’s where they want to be is better care than them dying attached to machines in an ICU that they never would have wanted. Coincidentally it’s also less expensive care.”
Less expensive than repeat trips to the emergency room, or a lengthy stay in an intensive care unit. The nation spends billions of dollars on care like this for patients during the last year of life. And a recent Institute of Medicine report found all that spending isn’t necessarily helping us live longer or better. Kelly McCutcheon Adams helps run the Conversation Project for the Institute for Healthcare Improvement in Cambridge, Massachusetts. She says it’s not that we should stop spending money caring for people in the last months of their lives. We should empower patients to choose how they want to live during the time they have left.
“The conversation ready work is not about limiting care, it’s not about there only being one pathway. And yet, what we do see is there are people who want to be at home, but aren’t.”
***
“My name’s Debbie. I live out in the country on 8 3/4 acres of land.”
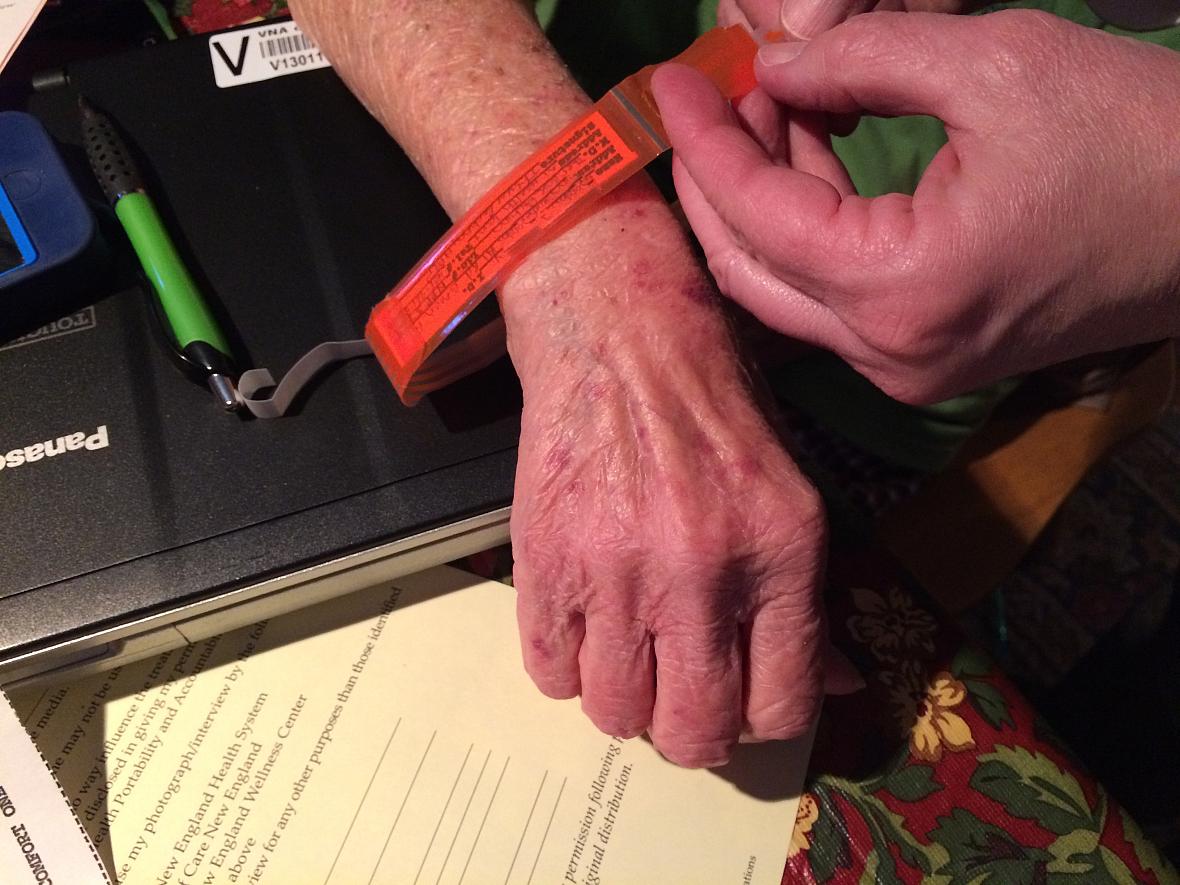
Debbie has advanced lung cancer. She doesn’t want to use her last name to protect her privacy. She’s sitting at her kitchen table, breathing oxygen through tubes. She’s here, at home, in part because of The Conversation Project. Her visiting nurse leans in to attach an orange plastic bracelet to her wrist that says “Do not resuscitate.”
For Debbie, the bracelet can declare her wishes if she can’t. And what she wishes is to enjoy the time she’s got left to live at home with her husband. It’s been a long road to this point. Doctors diagnosed her lung cancer a few years ago. They removed a tumor and part of her left lung. But after many rounds of chemotherapy and radiation, the cancer kept coming back. And the treatments made her weak and sick.
“I just got tired of every time me having a treatment, ending up in the hospital. I got tired of being in the hospital. So my husband and I talked. And I said, ‘I’m done.’”
Debbie says her doctors never gave her false hope, but they might have wanted to keep trying new treatments if she hadn’t made it clear she was done.
“You want the truth. You want to know where you stand. You want to know they’re going to back you and support whatever decisions you make.”
It took some difficult conversations with doctors and family to make those decisions. But Debbie’s wishes are clear now, strapped to her wrist, documented in her files. She’s written her own ending, even though it’s coming sooner than she wanted.