
Medicare penalties take heavier toll on hospitals with the most vulnerable patients
Created by the Affordable Care Act to cut costs and improve quality, Medicare’s penalty programs disproportionately impact hospitals serving the sickest and poorest patients.
Jenna Flannigan is a senior editor at Healthline.com and a freelance writer. This story was produced as a project for the 2015 California Health Journalism Fellowship, a program of the USC Annenberg School for Communication and Journalism.
Other stories in this series include:
Medicare Penalties: What causes hospital readmissions?


Medicare Penalties Take Heavier Toll on Hospitals with the Most Vulnerable Patients
In 1755, Benjamin Franklin helped choose Pennsylvania Hospital’s seal. It’s an image of the Good Samaritan inscribed, “Take care of him and I will repay thee.”
That hospital, the nation’s first, has been in continuous use since then.
Earlier this year, Joseph Alkus, a born-and-raised Philadelphian, was so pleased with the two spinal surgeries he received there that he wrote a letter of praise to the hospital’s executive director.
Alkus told Healthine that he regards himself as a discerning patient. He had considered another local hospital but felt uneasy about the surgeon.
Before his consultation at Pennsylvania Hospital, he saw his new surgeon listed prominently in Philadelphia Magazine — it clinched his decision.
What Alkus didn’t know was that the federal government has repeatedly penalized the hospital for quality issues.
The Affordable Care Act, more commonly known as Obamacare, created three separate programs that reduce Medicare payments to hospitals that don’t perform well on certain quality metrics.
In 2015, Pennsylvania Hospital ranked second in in the nation — out of more than 3,000 hospitals — for the total penalties it received, including one designed to target surgical errors and infections.
“If somebody had said, ‘You might have a higher chance of getting an infection at Pennsylvania Hospital,’ that probably would have impacted my decision to have surgery there,” Alkus said.
But some experts aren’t convinced that the hospitals receiving penalties are riskier places to seek treatment.
The penalty programs were intended to promote higher quality of care, along with lower rates of medical errors and hospital readmissions. However, early research suggests the program metrics may have flaws and some hospitals may be unfairly burdened with penalties.
The Hospitals Most Impacted
“No patient wants to get out of the hospital and feel like they were at a lemon,” Dr. Ben Raimer, vice president of health policy and legislative affairs at University of Texas Medical Branch (UTMB), told Healthline.
He added that, in an ideal world, the risk of medical errors would drop to zero.
Pennsylvania Hospital
But UTMB hasn’t reached that ambitious mark. Like Pennsylvania Hospital, it got dinged in all three Medicare penalty programs.
It’s also a storied institution, home to the oldest medical school in the Lone Star State. The hospital once offered its full range of medical services to any patient who came through its doors, including the uninsured, until mounting debt led to cutbacks.
One of the biggest criticisms of the Medicare penalty programs is their heavier impact on two types of hospitals.
One is the “major teaching” hospitals, which tend to care for the sickest patients. The other is “safety net” hospitals, which care for the poorest patients.
Take UTMB: It is a major teaching hospital because it runs a large education program to train new doctors. Since major teaching hospitals tend to have more specialists and advanced technologies, they generally care for patients who are sicker and require complex treatment.
For example, UTMB is the only hospital in the region with a trauma center, where a patient might be taken after a serious car accident. UTMB is also considered a safety net hospital because a hefty percentage of its patients have low incomes.
Medicare’s three penalties programs are all different — and each program has a heavier impact on hospitals like UTMB for different reasons. The penalties are based on data that aren’t current, so hospitals may have improved by the time they are penalized.
Here is a summary of each program:
- Hospital Readmissions Reduction Program (Readmissions): If a patient returns to the hospital too soon after discharge, it may mean the hospital didn’t provide good care in the first place. But research suggests patients from poor neighborhoods, and those in worse health, are more likely to be readmitted. Hospitals are penalized for higher-than-average rates of patients readmitted within 30 days—but only for some conditions, like heart failure and pneumonia. Penalized hospitals lose 3 percent of Medicare’s base payment for all in-patient care.
- Value-Based Purchasing (VBP): Paying for care based on volume of services may encourage doctors to order unnecessary tests. Medicare wants to pay for value, not volume. In this program, money that low-performing hospitals lose through penalties — up to 1.5 percent of Medicare’s base payments for in-patient care — creates a pool for high-performing hospitals to get bonuses. This year’s pool was about $1.4 billion. Hospitals are assessed on a complex set of quality measures. Major teaching and safety net hospitals are more likely to face penalties.
- Hospital-Acquired Conditions (HAC): In this program, the quarter of hospitals with the worst rates of certain infections and injuries receive a 1 percent cut to their total Medicare payments for in-patient care. Some experts are concerned the program is structured in such a way that hospitals doing the most to prevent medical errors are the most likely to be penalized.
The penalties in each program were designed to be small — but for some hospitals, they add up. Pennsylvania Hospital’s penalties were more than 4 percent. Like UTMB, it is a major teaching hospital with a high portion of low-income people. The hospital declined to comment for this story.
For UTMB, the combined penalties were more than 2 percent, translating into more than $2.5 million. Next to the hospital’s $1.5 billion operating budget, some would consider the penalty quite small.
Raimer disagrees.
“There was a time when people saw that as eraser dust. They’d just sweep it away,” he said. “What we live in now is an age where your margin is make or break for these hospitals. There’s no such thing as an insignificant penalty now.”
A Focus on Double-Duty Hospitals
Healthline conducted an analysis of Medicare’s 2015 penalties.
Out of the 3,000 hospitals subject to all three penalty programs, we focused on the small group of 159 hospitals that — like UTMB and Pennsylvania Hospital — serve as both major teaching and safety net hospitals.
Since these hospitals play dual roles in caring for the poorest and sickest patients, we call them “double-duty” hospitals.
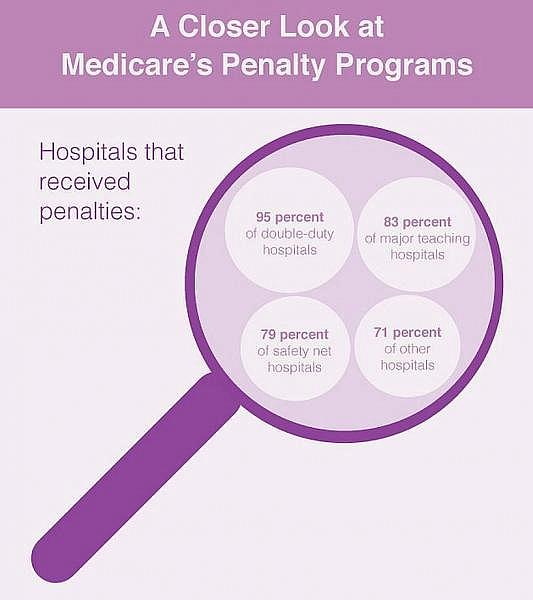
Our analysis found that more than 95 percent of double-duty hospitals received a net penalty across Medicare’s penalty programs. Most were fined in all three. By comparison, fewer than 75 percent of other hospitals faced net penalties.
There are many major teaching hospitals that do not serve large numbers of low-income patients — and many safety net providers do not have a teaching program. The penalties also had a disproportionate impact on those hospitals, but the biggest impact was on double-duty institutions.
The sum of the penalties was fairly small. Fewer than 30 double-duty hospitals received combined penalties of more than 2 percent. However, among that group were highly regarded institutions, including Yale-New Haven Hospital and New York Methodist Hospital.
Large, urban hospitals were also more likely to receive penalties. Thirty-two double-duty hospitals are located in New York City, a hub for medical education that has many high-poverty areas.
Healthline looked deeper at why each Medicare penalty program takes a heavier toll on double duty hospitals in these stories:
- Preventing Hospital Readmissions Among the Most Vulnerable Patients
- Medicare’s Search for High-Value Hospital Care
- Finding the Right Measures to Protect Patients from Hospital-Acquired Conditions
For a closer look at the medical facilities affected, visit our list of double-duty hospitals.
The Financial Impact on Hospitals
The U.S. healthcare system is the most expensive in the world, yet reports consistently show that quality of care is worse here than in other wealthy countries. Finding a way to cut costs while improving quality is the Holy Grail of healthcare policy.
Medicare’s penalty programs — also known as “pay for performance” programs — are one small part of that quest. As the nation’s largest insurer, Medicare has influence over the policies and financial stability of the vast majority of hospitals. Most hospitals couldn’t stay open without its payments.
That’s one reason it’s important for researchers to monitor the impact of the penalty programs on hospitals, Jason Hockenberry, Ph.D., an associate professor at Rollins School of Public Health, Emory University, told Healthline.
If one hospital continued to incur penalties on the higher end of the spectrum every year, Hockenberry speculated, “Even if it was a large hospital, that may be enough over the course of five years to put them in financial dire straits.”
Hospitals operating on tight financial margins have little room for error, said Dr. Christopher Cargile, chief medical quality officer at UAMS Medical Center in Little Rock, Arkansas.
“Any reduction in expected revenue really turns into fairly significant impacts on choices, staffing, programmatic planning,” Cargile said.
UAMS received penalties in all three programs, totaling about $1.8 million. It costs about $600 million to run the hospital, and it has faced budget deficits in recent years.
“The penalties may seem small relative to the hospital’s overall budget, but they may be the difference between breaking even or not,” Dr. Janis Orlowski, chief health care officer at the Association of American Medical Colleges, told Healthline.
At UTMB, Raimer said, “For us, $2.5 million more in our budget, I can tell you, would purchase us 30 more nurses. It would allow us to increase our school of nursing.”
However, some hospital administrators were less concerned about the financial impact.
“The penalties are not enough to really hurt per se,” said Imam Nazeeri-Simmons, chief quality officer at San Francisco General Hospital, which received slightly more than $500,000 in penalties. She described it as a “drop in the bucket” compared to the hospital’s operating costs.
But she noted that could change as government pay-for-performance programs grow, adding, “Every one of us realizes this is just the tip of the iceberg as far as the future of healthcare financing.”
Paying for Performance in Healthcare
Medicare’s pay-for-performance initiatives are expected to expand. In January, the federal agency set a goal to tie 90 percent of its payments to quality indicators by 2018.
The approach has already trimmed Medicare’s spending. In 2015, readmissions and HAC penalties alone saved nearly $800 million — funds that would otherwise have gone to hospitals.
But not everyone is convinced pay-for-performance programs will lead to cheaper, higher-quality healthcare.
A 2013 Harvard Business Review report noted the lack of evidence that such initiatives improve patient health and pointed to the failure of similar policies in education.
A recent Institute of Medicine study also raised concerns about the widespread use of quality metrics that are imperfect and hard to track.
Hospital administrators told Healthline they agreed with the idea of linking performance to payment. But many were concerned that Medicare’s penalty programs don’t account for factors such as poverty. They noted that their hospitals were competing with for-profit hospitals that don’t take high-risk patients.
No one knows at what point a hospital’s budget issues will compromise its ability to operate so much that quality suffers. Several studies have linked tight hospital margins to worse quality.
It’s the potential catch-22 of pay-for-performance programs. Facilities that might be the most in need of money to improve quality end up facing the highest fines.
“No matter which way you look at it, if we don’t have that money, it makes things more difficult for us,” said Thomas Thomson, director of external relations at St. John’s Episcopal Hospital in Far Rockaway, Queens, New York.
Located in one of the poorest neighborhoods in New York City, St. John’s became the only local option for most medical services after another hospital closed in 2011.
Like many on Healthline’s double-duty list, the hospital faced penalties in all three programs. It has also endured a string of budget crises in the past five years that included closing units, layoffs, sheltering people during Hurricane Sandy, and a cash shortage for day-to-day operations.
St. John’s has bigger budget concerns than the penalties, Thomson noted. But he said their “unfair impact” is still an issue.
On the other hand, some hospital administrators said the penalty programs had increased their hospitals’ focus on quality, which led to improvements in patient safety.
“It has been one of many leverage points for us to improve our quality and safety culture,” Cargile told Healthline. He added that at UAMS, they expect to cut their total penalties in half next year.
Nazeeri-Simmonds shared similar news about San Francisco General. The hospital expects to avoid readmissions and HAC penalties next year but to receive a small VBP penalty.
For others, the penalties may grow. Harris Health System, which runs the county safety net hospitals in Houston, Texas, received $100,000 in penalties this year. But Michael Norby, C.F.O. of Harris Health, said the penalties may go up to $500,000 in 2016.
Norby explained that a brief spike in patient safety issues was responsible for the potential increase in penalties. He added that Harris Health’s quality team had addressed those issues. He expected the penalties to shrink again by 2017.
High Quality Healthcare Is the Ultimate Goal
Administrators agree that quality of care in hospitals needs to improve. Infections and injuries related to medical care may cause up to 400,000 deaths annually. The question is how to reduce that number.
“Hospitals are spending enormous resources targeting specific quality metrics,” Cargile told Healthline. Medicare’s penalty programs are part of the reason that’s happening.
At the same time, those programs are disproportionately taking funds from hospitals that care for the poorest and sickest patients. For hospitals that can’t escape the cycle of being penalized, Hockenberry speculated the penalties might become meaningful.
At Harris Health, Norby said the ultimate goal is to get everything right from a quality perspective. But he didn’t expect that the health system would ever win big in pay-for-performance programs.
“As a safety net, there is just enough stacked against us,” he added.
[This story was originally published by Healthline News. The statistical analysis conducted for this story is available by request.]