
Birth Justice: The Fight for Reproductive Freedom in Indian Country
The article was originally published in The Imprint with support from our 2024 National Fellowship.


Shavonne Stevens at her Seneca Nation home in Cattaraugus, New York.
Photo by Malik Rainey for The Imprint.
On Thanksgiving Day 2020, Shavonne Stevens and her partner arrived at a hospital in Buffalo, New York, ready to meet their fourth baby — a moment that should have been filled with joy, hope and the tender magic of new life.
Instead, it felt more like survival.
Shortly after admission, Stevens learned her baby was “sunnyside up” in utero — a face-up position that can make labor longer, more painful and riskier for both mother and child. She had been laboring on her side, letting her body guide the baby into a safer position.
But when the nurse midwife arrived, the atmosphere in the delivery room shifted — like a freight train rolling in — and the birth that Stevens hoped for began to unravel.
“She took me by the legs and forced me on my back and said, ‘No, you need to push like this,’” Stevens, now 36, recalled.
Time slowed. The baby’s position in the birth canal made each contraction more grueling, sending pressure and pain ripping through her lower back and thighs as the baby’s skull pressed against her tailbone. Heart pounding, Stevens was trapped in a position that defied her natural instincts.
When her daughter, Denver, finally emerged, she was injured from passing face-up under the pelvic bone.
“Her face was swollen, her forehead and nose were black and blue, and she was looking up at the stars,” Stevens said. “She probably wouldn’t have been born like that if they would’ve let me labor how I wanted.”
Adding to the stress, Stevens said the postpartum nurses were rude, and no one came to help her breastfeed: “They basically ignored us and kept trying to push the bottle, which I wasn’t going to do.”
Stevens wanted dignity, care and connection in an environment where she felt respected and safe. But after enduring four hospital births that were marked by disregard and thinly veiled contempt, she vowed never to return to the hospital.
Stevens’s experience is not uncommon among Native women in the United States, who have survived centuries of prejudice, indifference, neglect and medical abuse by their providers. As a result, they now experience the worst per capita maternal health outcomes in the country during pregnancy, labor, delivery and postpartum.
Her story reveals the challenges tribal members face giving birth — and also the ways tribal communities are reclaiming maternal health care on their own terms. Stevens and countless other American Indian and Alaska Native women are challenging the status quo, turning their collective anger at these ongoing inequities into a demand for accountability, adequate funding, data visibility, and the right to safe, respectful and culturally informed birth experiences.
Native women are challenging the status quo, turning their collective anger at these ongoing inequities into a demand for accountability, adequate funding, data visibility, and the right to safe, respectful and culturally informed birth experiences.
Across Indian Country, this growing birth justice movement is driven by a range of Native-led initiatives, involving advocacy organizations, Indigenous midwives and doulas, and grassroots maternal health programs — the Alaska Native Birthworkers Community, Tewa Women United, Changing Woman Initiative and the Indigenous Birth Justice Network, to name a few.
“Midwives are being trained in our communities because of the desperate state of maternal and child health across the U.S,” said Katsi Cook, a midwife and member of the St. Regis Mohawk Tribe at Awkwesasne in upstate New York. “The opportunity is for us to realize our own strength and our own power in building something that comes from the inside — not the outside.”
Origins: The birth of a continent
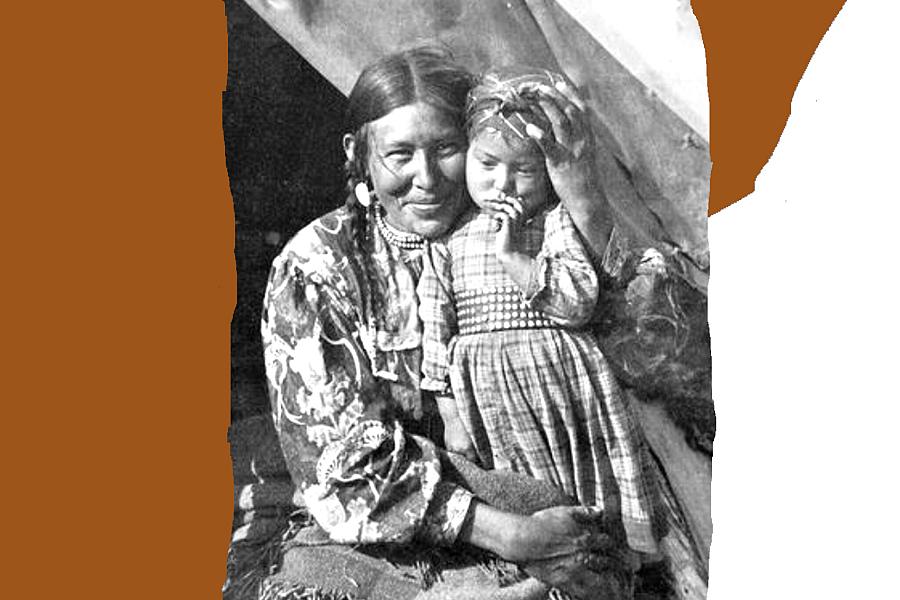
An Indigenous mother and child photographed in the early 1900s when federal officials and government physicians were focused on regulating Indigenous reproduction.
Photo by Edward S. Curtis, Library of Congress.
Indigenous women gave birth to an entire hemisphere.
For thousands of years, birth was attended by midwives, grandmothers and female relatives with ceremony, prayer and collective support for mother and baby. Though each tribe had its own customs, the arrival of a child was a sacred event that included family and community in an unbroken cycle of life that promised continuity for generations to come.
In many tribal societies, ceremonies for a woman entering puberty were a time of celebration which brought her into the circle of midwives and elder women who would help deliver her children, as well as mentor and guide her throughout her life.
From the Arctic Circle to the tip of southern Chile, midwives used sophisticated knowledge of birth, healing and traditional medicines that strengthened and sustained their communities for millennia. When Christopher Columbus arrived in the late 15th century, experts estimate that approximately 90 to 112 million people inhabited the Western Hemisphere.
By the early 1600s, however, experts estimate that 95% of the Indigenous population perished due to disease, conflict and colonial expansion.
Unequal access: The maternal healthcare crisis in Indian Country
Beginning in the early 20th century, as the pseudoscience of eugenics gained influence around the world, Native American women were targeted for sterilizations and their children were forced into boarding schools and foster care. These policies were intended to suppress and reduce Native population growth and erase Indigenous cultures.
The impact was immediate and devastating. A sweeping 1928 federal investigation, known as the Meriam Report, found that in Montana alone the infant mortality rate in 1927 among Native Americans was 185.4 per 1,000 births, compared to 69.1 for whites.
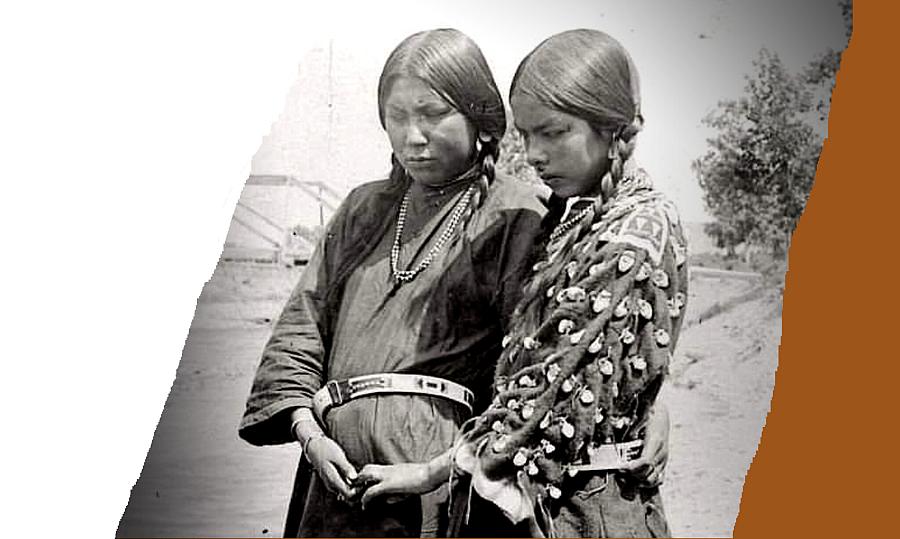
Two pregnant Indigenous women photographed in the early 20th century. In the decades that followed, federal policies shaped by eugenic ideology increasingly targeted Indigenous women’s reproductive lives.
Photo by Edward S. Curtis, Library of Congress.
Maternal mortality also spiked. By the early 1940s, Navajo mothers, for example, had an estimated mortality rate of approximately 1,000 deaths per 100,000 births. That was nearly four times the U.S. average of 270 per 100,000 at that time, according to a 1990 study published in Medical Anthropology.
Modern barriers have further exacerbated this crisis. Pregnant tribal members face chronic shortages in care, including understaffing, long wait times, limited access to specialists and emergency obstetric care and fragmented coordination between tribal, state and federal health care systems.
Alaska Native women are routinely forced to travel hundreds of miles by seaplane for prenatal care and childbirth — often alone and without family support. In a state two and a half times larger than Texas, where many communities are accessible only by air or water, weather, geographic isolation and travel delays can quickly become medical emergencies.
These factors have led to a maternal health care crisis in which Native women die of pregnancy-related complications at rates of up to 10 times higher than their white counterparts in some states, according to the Journal of the American Medical Association.
A new generation of midwives
Now, an Indigenous-led grassroots movement is confronting this systemic failure by reclaiming birth sovereignty. The work is led by Native midwives and doulas, lawmakers, clinic directors, activists and researchers in states including Alaska, Washington, New Mexico, Arizona, Oklahoma, North Dakota, Minnesota, Wisconsin, New York and others.
Their efforts include building ceremonial birth lodges and tribal birthing centers, facilitating home births and restoring reliance on traditional medicines and birth practices. Services include pre- and postnatal clinical and cultural support, patient advocacy within health systems, mental health services, accompanying mothers to medical appointments, and holding in-person and virtual workshops and sharing circles — community-driven initiatives restoring Indigenous knowledge and practices. Practical needs are also being met by local initiatives, providing basic necessities and postpartum items like diapers, wipes, car seats and breast pumps.
A social media graphic from the Canada-based National Council of Indigenous Midwives highlights the resurgence of Indigenous midwifery.
Graphic from Indigneousmidwifery.ca.
In the face of chronically underfunded federal health systems, geographic isolation and jurisdictional barriers, these caregivers are helping reduce maternal and infant mortality rates and restoring dignity to birth in tribal communities, according to the National Indian Health Board.
Katsi (pronounced Gudji) Cook is a member of the St. Regis Mohawk Tribe at Akwesasne, New York. She has been at the forefront of restoring Indigenous midwifery nationwide for nearly half a century. A founding member of the National Council of Indigenous Midwives, she began practicing as a midwife and advocating for Indigenous maternal health in the 1970s, shaping policies that bridge traditional birthways with public health research and human rights efforts for American Indian and Alaska Native families.
Katsi Cook
Cook’s prenatal approach integrates both clinical care and traditional medicine, encouraging her patients to follow the guidance of elders and other mothers.
“Many Indigenous women are alone and disconnected with no mother, father or family to support them,” Cook said. “But if you don’t have a mother, find someone to sit in her place, an auntie or friend — because even if it’s a conversation about ‘How did you do this?’ it can still be so powerful.”
She also encourages Native women to know their health data and be prepared to advocate for themselves at medical appointments.
“They need to show up with knowledge. Every woman should know her hemoglobin, A1c, blood pressure — all of the biomarkers, because that’s what the clinicians are going to look at and judge you by because of the racism that’s inherent in the structure of those systems,” Cook said.
Cook said home births are experiencing a resurgence across Indian Country due largely to the individualized care and respect provided by “new generations of midwives in our own communities.”
She describes traditional birth as an act of resistance. But that resistance requires more than awareness, she added. It calls for integrating traditional ways of giving birth with practical medical knowledge that preserves community continuity and intergenerational wisdom.
Many Native women, for example, report being subjected to unnecessary interventions — including drugs to induce or speed labor, episiotomies, epidurals and Cesarean sections without clear medical necessity or informed consent.
We didn’t forget that knowledge. We stopped doing it, and knowledge comes back through the doing.
Katsi Cook
Cook believes that true empowerment means trusting women to listen to their own bodies, rejecting unnecessary medical procedures and embracing practices rooted in tradition and personal choice. She advocates for the inclusion and active participation of family members in birth spaces, who are often left out and dismissed by Western practitioners.
“What was missing wasn’t culture — it was knowledge of our own bodies, our spirit, our relationship to creation,” Cook said. “We didn’t forget that knowledge. We stopped doing it, and knowledge comes back through the doing.”
A powerful decision

Shavonne Stevens, seen here at home, says learning from Indigenous birth workers was transformative and made her feel empowered.
Photo by Malik Rainey for The Imprint.
Struggling postpartum in early 2021, Stevens began searching the Internet to seek help. She stumbled on something called a “postpartum doula,” which was a completely new concept for her.
“I didn’t even know what a doula was, and why had I never heard of this?” Stevens said. “So I looked into it and signed up for a class.”
Discovering the world of Indigenous midwifery, doulas and home birth was a revelation. Having had four hospital births, “I thought I knew everything,” she recalled. “But I didn’t know anything.”
As I was learning from them about birth and postpartum, which they taught from a traditional perspective, it all made sense.
Shavonne Stevens
During her doula training, Stevens found a home among other Native birth workers who center pregnancy in their communities by including elders, friends and family, preparing and using traditional plant medicines, and observing cultural protocols during gestation and birth.
Midwives and doulas from the Six Nations Birthing Centre in Ontario, Canada, and Akwesasne, New York, took her under their wing, teaching her the traditional practices for childbirth that guided the women of the powerful Iroquois Confederacy — known collectively as the Haudenosaunee in their language — for thousands of years.
These birth workers are restoring traditional knowledge, strengthening community bonds and returning agency to Native women.
Learning from these women, Stevens said, felt transformative — acts of ancestral remembrance that made her feel empowered.
“These women talked very positively about their home births, which I had never heard before,” Stevens said. “As I was learning from them about birth and postpartum, which they taught from a traditional perspective, it all made sense.”
The Native birth justice movement had finally found her, awakening a fierce determination to reclaim traditional Haudenosaunee birth practices — not only for herself, but also for her community.
Building a policy road map for Native maternal health reform
Across Indian Country — from tribal lands to urban centers — community-based leaders are at the forefront of a nationwide effort advocating for legislation and policies that expand access to care and confront persistent disparities in Native maternal health.

Nicolle Arthun
Nicolle Arthun is the founder of Changing Woman Initiative, a nonprofit serving Indigenous women in Albuquerque, New Mexico. An internationally recognized certified nurse-midwife, she has spent decades advocating for tribal maternal health by working to reclaim traditional birth practices and restore Indigenous midwifery rights.
As one of the preeminent voices in maternal healthcare reform for American Indian and Alaska Native women, Arthun established Changing Woman in 2015 after getting her masters in nurse-midwifery at the University of New Mexico. Her motivation was driven in part by her own birth experiences, and by observing the mistreatment of Native American women and their families by other medical professionals when she was a young nurse at the Santa Fe Indian Hospital.
“Women in labor were shamed for asking for epidurals, or told to ‘shut up’ by their nurses if they cried too loud,” Arthun said. “I would overhear the non-Native staff make negative comments about these women and saw how they treated them with disrespect, which is one of the big reasons I felt I had to do something.”
Arthun said she was alarmed by the way Native women are treated in health care settings.
“They don’t know what their rights or options are or what they can say yes or no to,” Arthun said, “because providers expect them to do what they are told.”
As a 2024 fellow with the Robert Wood Johnson Foundation Health Policy Fellowship, she’s been working with New Mexico U.S. Sen. Ben Ray Luján to develop a national strategy for improving maternal health outcomes for American Indian, Alaska Native and Native Hawaiian women.
I would overhear the non-Native staff make negative comments about these women and saw how they treated them with disrespect, which is one of the big reasons I felt I had to do something.
Nicolle Arthun
This landmark effort is the first of its type in nearly 250 years of federal Indian policy, and centers on five comprehensive policy briefs which outline solutions to maternal mortality, workforce equity, access to health care services, Indigenous data sovereignty, and funding inequities. The policies were developed by tribal members and 55 maternal health experts. They provide a devastating picture of the maternal health crisis in Indian Country — and solutions for addressing it.
Released by Luján’s office last December, the reports are intended to guide legislation that will improve maternal health outcomes in Indian Country.
“For far too long, Native families have had to be subjected to a maternal health system that was never built for them. These reports offer a roadmap that is based on data sovereignty, community-led care, and sustained federal investment and support,” Sen. Luján said in an emailed statement.

Sen. Ben Ray Luján
“I look forward to seeing many of these solutions put to work and to making things better for Native mothers and care facilities.”
But efforts to secure additional funding to address the Native maternal health crisis are now under threat due to the ongoing budget conflicts in Congress — which led to the longest government shutdown in U.S. history last fall.
In January, legislators passed a bipartisan, bicameral “minibus” appropriations package to avert another government shutdown by providing full-year funding for several federal agencies and programs.
For Indian Country, this funding includes Indian Health Service and other maternal, behavioral health and community-based services that many Native families rely on as their primary — and often only — source of care. But Arthun and other advocates argue that funding levels and sustained investment in maternal and infant care still fall far short of what is needed to adequately address persistent disparities, workforce shortages, and the unique geographic and jurisdictional barriers facing tribal communities.
“The maternal health crisis in Indian Country is an invisible issue that can no longer be overlooked,” Arthun said. “We’re done waiting for change and we are prioritizing our women and children through engaging with Congress for long-term solutions, policies and funding that are strategic to advancing our continued survival as tribal nations.”
For Native women, the challenge goes beyond availability of care, she added. Without targeted investment and ongoing, consistent support, “future generations will feel the outcomes of the decisions made today — which will have long-term impacts.”
A new beginning and a farewell

Back home on Seneca territory in Cattaraugus, New York, Stevens is now the mother of six — four girls and two boys. Her last two children were delivered at home. Stevens says her home births were a healing contrast to her hospital deliveries, defined by love, ceremony and community support in a way that reflected her family’s traditional Seneca beliefs.
Her sixth child, a daughter named Baela, was delivered with her partner by her side in January 2025. Her birth plan included three traditional Seneca doulas and a midwife.
It was the old way and it was so calm and beautiful — every birth should be like that.
Shavonne Stevens
“I needed all the support I could get with five other kids in the house,” she said. “I needed a doula for me, a doula for the kids and someone who was praying over me and thinking good thoughts.”
It was a traditional Haudenosaunee birth.
“I breathed her out and held her close and it was important to me for her to hear only Seneca when she came out,” Stevens said. “In our culture, no one speaks until we speak first, so I announced that it’s a girl — Godöni’a:h — in Seneca.”
A short time later, the doula came in, greeting the baby in Seneca before offering the welcoming speech and singing the traditional “Baby Song” to Baela.
“It was so emotional,” Stevens said. “It was the old way and it was so calm and beautiful — every birth should be like that.”

Stevens after giving birth at home to her daughter, Baela.
Photo by Kaylei Miller Photography.
From these deeply personal birth experiences at home, Stevens’ work has blossomed into a commitment to supporting mothers and nurturing newborns in her community.
Now a certified doula and lactation consultant, Stevens said she has lost count of the number of Seneca women whom she has attended during birth or helped with breastfeeding. She is on a mission to help train more Indigenous doulas while continuing to restore traditional Haudenosaunee birth practices to their rightful place.
But one sacred task remained — a final act that brought her birth journey full circle.
“They say to plant your placenta with the cord down, which tells the connection with the Earth that you’re done having children,” Stevens said. “If you plant it cord up, then that tells the Earth that you want more.”

Stevens, center, with her mother and her six children, is now a certified doula and lactation consultant. Her last two children were delivered at home.
Photo by Malik Rainey for The Imprint.
In July 2025, Stevens held a traditional placenta ceremony near her home in Cattaraugus. Surrounded by her six children, they found a spot in the woods where they smudged and dug a small hole.
Taking Baela’s placenta in her hands, Stevens placed it, cord down, along with the placenta cords of her other five children. She covered them with dirt, as her children laid flowers, prayed and gave thanks to the Creator. Like hundreds of her grandmothers before her, she returned them to the Earth.
Wiping tears, she felt relief in reclaiming her traditional birth ways and finding her calling along the way — and a gentle ache knowing that Baela would be her last. In a moment filled with love and tenderness, she had passed down this ancient ceremony to her children.
Quietly, they gathered for a hug and slipped away to gather wild strawberries, carrying the ceremony and its lessons with them into the forest.
