The Paweleks lost their primary income. They also lost their health insurance — and the robust health care access it afforded. In other parts of the country, Mike’s disability insurance and Patty’s Obamacare plan could have easily gotten them a primary care doctor. But in mining communities like Elko County in northeastern Nevada, mine insurance is so important to the local health care infrastructure that many without it have to fight for basic care.
“We mostly had Newmont insurance forever and didn’t really know anything else,” said Patty, a 59-year-old retired school bus driver. “And then it just came all crashing down.”
Mike (left) and Patty Pawelek (right) leaned on the mine-run clinic to help Mike coordinate his care when he got sick, only to be turned away after he went on disability.
Courtesy of Patty Pawelek
The Paweleks’ struggles are emblematic of the problems that beset mining communities where health systems have been disrupted and distorted by the industry’s booms and busts, creating ripple effects that make it harder for people to access care, deepening inequities and worsening health outcomes in populations often predisposed to poor physical and mental health.
Mining companies offer good jobs with good benefits that can counterintuitively damage health care access. Health systems can grow dependent on those insurance plans to survive, and the benefits are in some cases so good that providers are reluctant to serve others in the community. It’s the consequence of a national health care system that feeds off employer-sponsored health insurance to turn a profit, and, as a result, warps itself to meet the needs of those who have it.
Six months of interviews with more than 90 patients, providers, retired miners, community leaders and health care experts across the U.S., including in three towns characteristic of the mining industry’s past, present and future — Williamson, West Virginia; Elko, Nevada; and White Sulphur Springs, Montana — reveal the breadth of these perils: retired and injured miners, and their families, struggling to get care; communities left with beleaguered or closed health facilities; and pricy hospital bills in towns where mines have driven up median incomes.
A growing number of communities will likely soon face similar predicaments as mines open across the United States amid the Biden administration’s push for more domestic sourcing of resources — such as copper, lithium and cobalt — needed to power electric cars and produce renewable electricity.
Copper, for example, is used in wind turbines, generators and electrical cables, and U.S. demand for the mineral is projected to double between 2021 and 2035. The Biden administration for the first time this year added copper to the U.S. critical materials list and is pushing to increase the domestic production and refinement of critical minerals and materials as it aims to achieve 100 percent carbon pollution-free energy in the next dozen years.
“It’s unclear yet how many new mines we’ll get in the United States. But we’ll get several, at least. Maybe a lot, and every one of those mines is going to be located in a community that’s going to have a pretty similar set of struggles,” said Mark Haggerty, senior fellow on the energy and environment team at the left-leaning Center for American Progress. “The challenge is going to be the same in all of these rural communities. They’re all going to have struggling health care, rural hospitals, potentially.”
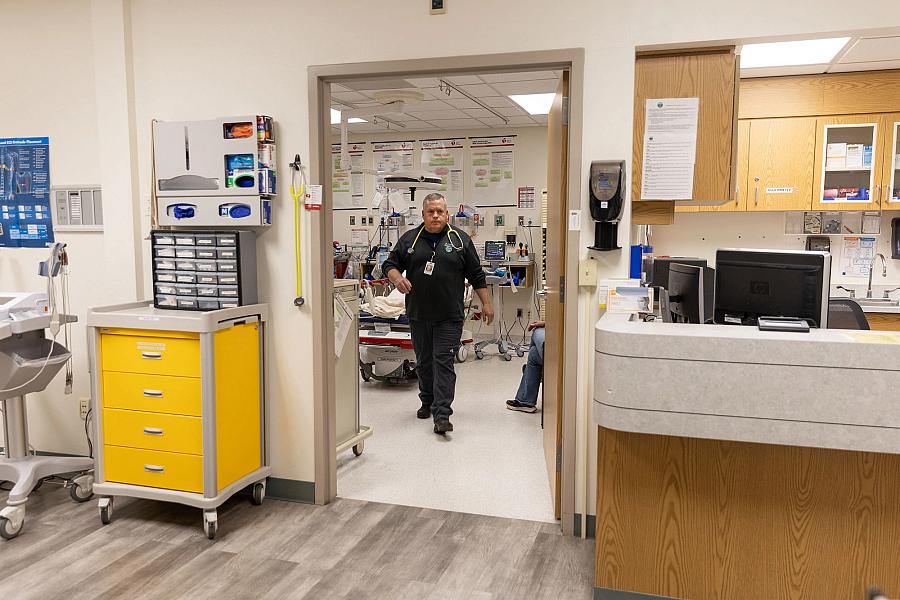
Physician assistant Scott Meissner (left), radiologic technologist Jayme Svejkovsky (center) and Dr. Adam Stenseth (right) work in the emergency room at Mountainview Medical Center. Mining associations in Montana and Nevada said good health plans reflect the talent of and risk to their workers, but acknowledge the unintended consequences.
Janie Osborne for POLITICO
Miners are more likely to have private health insurance than many other rural workers, in part, because of the dangers of the job. Nearly three-quarters of non-managers are insured by private health plans compared with roughly 57 percent in construction and 53 percent in agriculture, according to the Rural Policy Research Institute.
But these health plans are often better than the insurance in the rest of the community and create market dynamics that sour health care access.
“Doctors want these big reimbursements from the very rich insurance policies that the gold mine provides. They don’t want the pennies they receive from Medicare,” said Jan Brizee, former ombudsman for the Nevada Office for Consumer Health Assistance representing Elko and other rural counties. “So you have somebody who’s retired after 25 or 30 years, and now they have nothing, having to travel out of town to get even primary care, let alone a specialist.”
Key Takeaways
- The commercial health plans offered to mine employees typically reimburse hospitals and doctors at higher rates than Medicare and Medicaid.
- Miners’ good-paying insurance can destabilize the health care infrastructure in rural towns because the benefits are much better than the coverage the rest of the community has.
- That can leave retired and injured miners, as well as other residents, struggling to get care and jeopardize hospital stability.
- Medicaid expansion, extra federal funding to support health centers and critical access hospitals, and other policy solutions targeted at rural communities have in some cases helped but are often inadequate.
- A growing number of communities are expected to face these challenges amid a push by the Biden administration to mine and process more critical minerals and materials domestically to support the renewable energy transition.
Not all mining communities experience these problems, and similar issues exist in towns dependent on other industries with good benefits, like manufacturing. But mining communities face unique obstacles compared with other one-company towns — including remoteness and challenging geography — that make it difficult to attract other businesses that would diversify their health insurance landscape.
Miners also tend to be in worse health than their counterparts with other manual labor jobs, with higher rates of poor sleep and heart disease. And while mine-related injuries have dropped over the last decade, thousands of mine workers are still injured seriously enough each year that they miss work, according to the National Safety Council. Underground mining machine operators rank among the top 10 for deadliest professions, according to the U.S. Bureau of Labor Statistics.
The mining association in Montana said good health benefits reflect the risk and difficulty of the job, and Nevada’s mining association acknowledged that their robust benefit packages can have unintended consequences.
“The Nevada mining industry is proud of the benefit packages that are available to our employees. We also pay the highest wages on average among private employers — nearly twice the state average — and recognize that these robust compensation packages have a ripple effect through a community,” said Dana Bennett, interim president of the Nevada Mining Association, in an email.
The National Mining Association and the American Exploration and Mining Association declined to comment.
Medicaid expansion and extra federal funding to support rural health centers and hospitals have helped in some towns. But providers bemoan stingy state Medicaid reimbursement rates that aren’t enough to pay the bills, paltry federal funding to support primary care and hospital designations that don’t meet the needs of all facilities.
For the most part, these solutions have inadequately addressed the systemic failures of employer-based health systems in these communities.
“It’s a huge, hidden sector of the American economy. It’s out in the hinterlands. No one in America knows,” said Michael Topchik, national leader at the Chartis Center for Rural Health. “These are communities that are meeting vital needs. But guess what? They have vital needs. Health care is one of those vital needs, and it’s failing.”
Known as the “the heart of the billion-dollar coalfields,” downtown Williamson was once perennially packed.
PART 1: WILLIAMSON
Before the floods, before coal crashed, before the opioid epidemic — and before it lost its hospital — Williamson flourished.
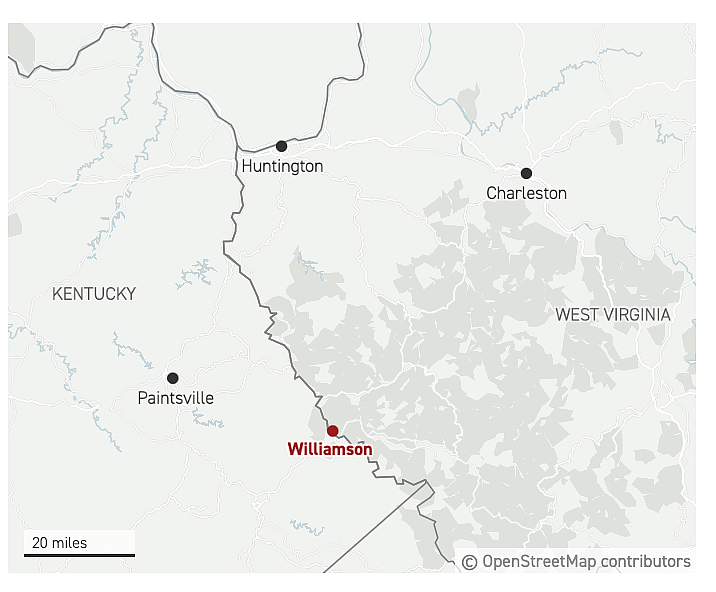
Known as the “heart of the billion-dollar coalfields,” downtown Williamson was perennially packed. People traveled 80 miles — from Charleston and Huntington, West Virginia’s two biggest cities — to shop, paying for everything with the wads of bills in their pockets.
And they came from all over the region to go to Williamson Memorial Hospital.
Most everyone in town has a story about the hospital on the hill. They were born there, or their kids or parents were. It saved them from pneumonia or complications from chickenpox or liver disease. People went to the cafeteria just for the chicken tenders.
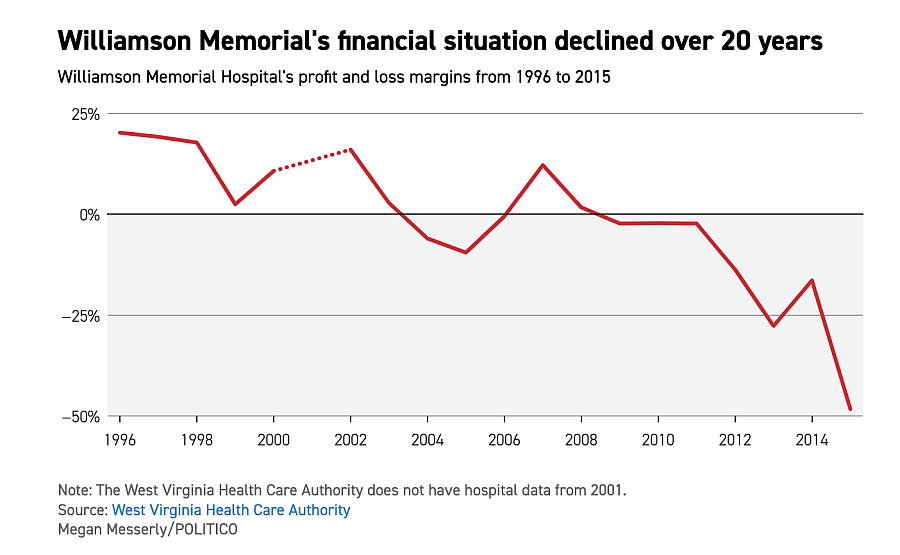
That was before coal collapsed, taking Williamson Memorial along with it. By the 1970s, increasing mechanization and more surface mining requiring fewer workers had diminished the coal workforce. And the industry tumbled into a death spiral after the Great Recession, the result of lower natural gas prices and a shift toward renewable energy. It hurt related sectors, like rail, too.
For decades, the hospital thrived on the industry’s good-paying health insurance, but it became so dependent on those plans it couldn’t survive without them.
“Once those health benefit plans went away, so did the access to health care,” said Nathan Brown, a lawyer, former coal miner and president of the Mingo County Commission.
‘A rippling effect’
Williamson is one of many rural Appalachian towns where the decline of the coal industry upended the health care system. The town is a shadow of its former self, and the closure of its lone hospital is a cautionary tale for communities anticipating the bounty new mines will bring.
“That hospital … offered stability to the community, and when those doors closed for the last time, it was another dent in the armor of our community,” said John Mark Hubbard, a former Mingo County commissioner whose father and grandfather were coal miners.
When coal was booming, companies paid 100 percent of health care premiums. Health plans were — and in other mining communities still are — an attractive benefit for workers.
“The amount of dollars company-wide that were appropriated to those health benefits 20 years ago was astronomical,” said Leasha Johnson, a former coal company employee and now executive director of the Mingo County Redevelopment Authority. “I had 100 percent coverage. The health care coverage was just phenomenal back in the heyday.”
The hospital had so much demand that it added a fourth floor and tripled the size of its emergency room in the mid-1990s. The facility boasted in the local newspaper of its robust suite of services, including two delivery rooms, three operating rooms, a seven-bed intensive care unit, a 16-bed telemetry unit, an endoscopic lab and a cardiopulmonary rehabilitation program.
Williamson Memorial and its sister hospital were so flush with cash that they funded the acquisition and construction of at least 30 hospitals across the southeastern United States, Dr. Dino Beckett said.
Dr. Dino Beckett, who was born and raised in town, said Williamson Memorial was so profitable that it and its sister hospital in Paintsville, Kentucky, another coal town, formed the financial foundation to grow Health Management Associates, the out-of-state hospital chain that acquired it in the 1970s. The two hospitals funded the acquisition and construction of at least 30 hospitals across the southeastern United States, Beckett said.
But the profits from coal’s heyday were not reinvested into the community, a third of which today lives in poverty.
“We have not benefited historically from the wealth that has been provided out of the resources that we have in southern West Virginia to prepare for the times we’re in today,” Hubbard said. “There wasn’t a lot of forward-thinking people.”
The West Virginia Coal Association did not respond to requests for comment.
Two of the hospital’s former CEOs said there’s nothing the facility could have done to prepare for coal’s collapse.
“I can’t think of a tactic that you could offer that would keep you going,” said Tim Trottier, who was CEO from 2000 to 2003. “The notion that you would still have a hospital if it’s not profitable is just not realistic.”
David Pryor, who ran the hospital in 2012, said there’s never an opportunity to stash money away with how expensive small hospitals are to run.
Declining jobs meant declining benefits. Declining benefits meant hospital challenges. Williamson Memorial’s parent company, Community Health Systems, sold the hospital to a local group in 2018 after the facility became insolvent.
The hospital filed for bankruptcy the following fall. By spring, Williamson Memorial had joined the nearly 200 rural hospitals that have closed in the last two decades.
The amount of dollars company-wide that were appropriated to those health benefits 20 years ago was astronomical
Leasha Johnson, a former coal company employee and now executive director of the Mingo County Redevelopment Authority
Hospitals in southern West Virginia have faced similar difficulties. Jim Kaufman, president and CEO of the West Virginia Hospital Association, said only about 13 percent of hospital patients have commercial health insurance in the eight counties where the bulk of the state’s surface mining took place, a number that’s dropped nearly 5 percentage points over five years.
“You may lose an employer in a large city or a suburban community, but they may account for a small percentage of your overall commercial population,” Kaufman said. “In a small town in West Virginia, one employer could be 50 percent. It could be a significantly large number, and then if you think about all the ancillary services that that mine provides, it has a rippling effect.”
A view from Williamson Memorial Hospital is shown. Williamson Memorial’s closure left Mingo County without a hospital for the first time in over a century.
‘Nails in a coffin’
By the time the hospital shut its doors, the town had been decimated by disasters — natural and human-made. Two floods washed away downtown businesses. The city lost its high school in 2011 when four of the county’s high schools were consolidated into one, 30 minutes away on reclaimed mine land. More recently, the town became one of the epicenters of the opioid epidemic: Drug wholesalers sent nearly 21 million painkillers to the town of about 3,000 over a decade, according to an investigation by the House Committee on Energy and Commerce.
Walk down Second Avenue and many downtown storefronts are vacant. Structure fires, usually related to people living in abandoned buildings, are common. Even Goodwill shut its Williamson store in 2017.
“It does feel like nails in a coffin,” said Dr. Steve Wilson, an optometrist. “You see your city identity really changed.”
Williamson Memorial’s closure left Mingo County without a hospital for the first time in over a century. Some cross the river to go to a hospital in Pike County, Kentucky, but that facility is out-of-network for others, including those covered under the health plan for state employees, who may drive more than 80 miles for in-network care. Covering those transportation costs can be a tall order when gas prices are rising, inflation is eating into household budgets and the median household income in town is $35,000.
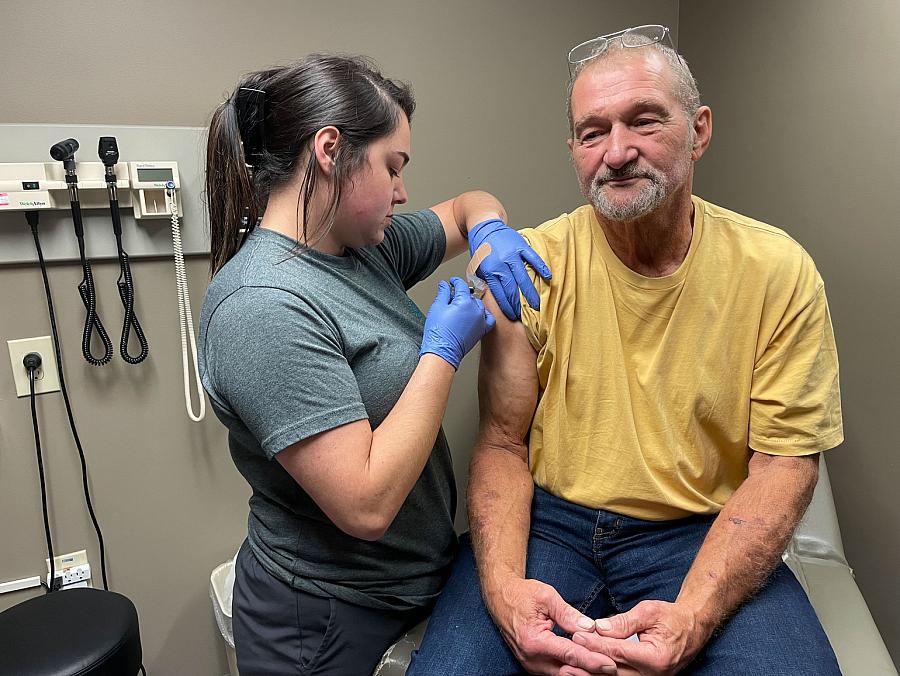
Autumn Gibson (left), 23, a nurse at Williamson Health and Wellness Center administers the flu shot to a patient. Williamson Memorial was purchased by Williamson Health and Wellness Center.
“You can’t always take off work and travel two hours to have things done, especially if you’re an hourly employee. It’s just not feasible for your family,” said Chris Dotson, president of the Tug Valley Chamber of Commerce.
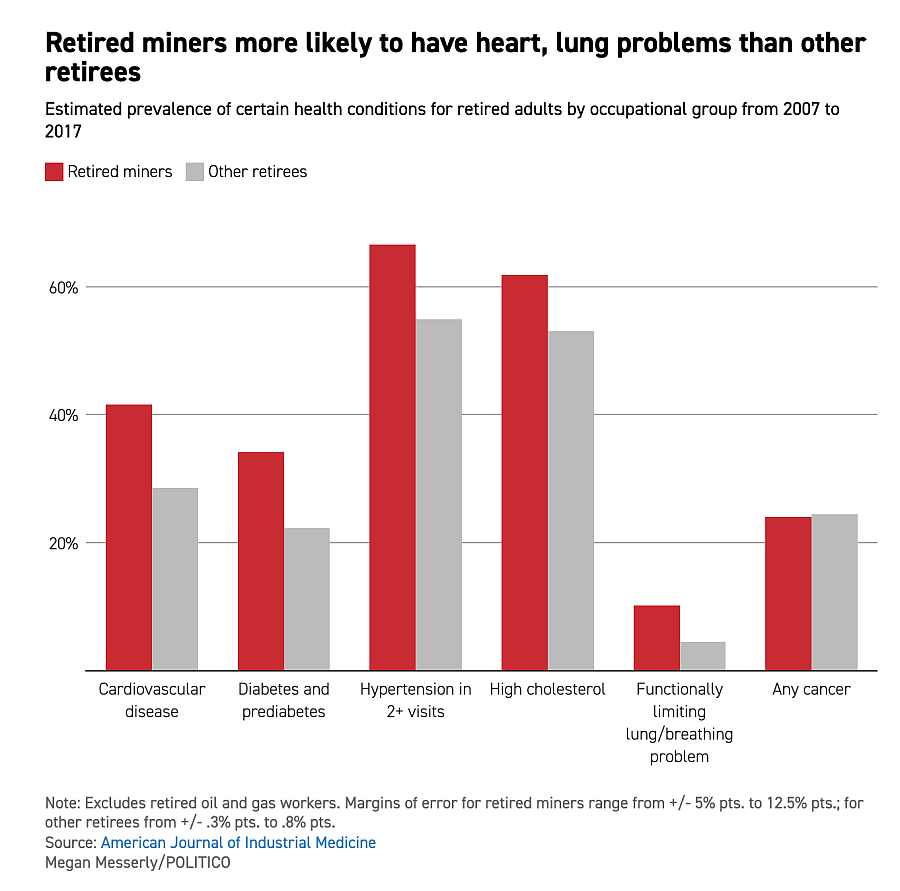
While the population has dropped by a third over the last three decades, there are still nearly 23,000 people in Mingo County, including many retired coal miners who struggle to access care. They are grappling with serious health conditions that include, but extend beyond, black lung disease, the incurable condition caused by inhaling coal dust.
“Those coal miners still exist in our community, and they have multiple health problems from years and years of working in the mines, whether that’s pneumoconiosis, black lung, COPD, heart disease — or, honestly, even some of them have bad arthritis that has to be treated,” said Karen Bowling, former secretary for the West Virginia Department of Health and Human Services and CEO of a hospital in Princeton, West Virginia. “We’ve got to find ways to support these individuals who, for their entire lifetime, have given back to this country by producing coal.”
A 2020 study from researchers at the National Institute for Occupational Safety and Health found that miners — coal and otherwise — have a higher prevalence of almost all health risk factors compared with most other manual labor workers, such as excessive alcohol use, chewing tobacco and sleeping less than seven hours.
After it closed, Williamson Memorial was purchased by Williamson Health and Wellness Center, a federally qualified health center. Over more than a decade, the health center has grown to encompass several downtown buildings and offer primary, pediatric, dental and behavioral health care. It even runs an indoor farmer’s market and plans to reopen the town’s beloved hospital.
Top left: A new CT machine is shown. Top right: An unrenovated room is shown. Bottom: The Williamson Memorial Hospital is shown. Renovations to the old hospital have been plagued by delays.
But renovations to the hospital have been plagued by delays. The reopened hospital also won’t qualify for additional federal funding, in part because it’s too close to the Kentucky hospital.
Beckett, who is CEO of the FQHC and Williamson Memorial, hopes the clinic will provide the hospital with a ready-made patient base that will support it financially. The hospital plans to start offering lab and radiology services by the end of December and inpatient hospital care after the first of the year. Emergency room care, the most expensive to provide, will begin later.
A patient room at Williamson Memorial Hospital is shown, with the old hospital building seen through the window. “Everybody in this town is waiting on this hospital,” said Larry New, a pharmacist at Hurley Drug.
For now, Williamson waits.
“Everybody in this town is waiting on this hospital,” said Larry New, a pharmacist at Hurley Drug. “If that hospital doesn’t make it, it makes you wonder if this town is going to make it.”
Elko’s challenges exemplify how good-faith efforts by mines to offer robust health benefits can unintentionally warp a town’s health system and create unusual market dynamics that hamper access.
PART 2: ELKO
Ask most anyone in Elko, and they’ll say they’re frustrated with their health care.
There’s the Paweleks, who leaned on the mine-run clinic to help Mike coordinate his care when he got sick, only to be turned away after he went on disability.
There’s also Janet Baker, 70, who relies on urgent care but knows she is “one little boo-boo away” from needing a primary care doctor. Sharae Grogan, 59, can’t find a doctor who takes her insurance, and the urgent care doesn’t either. And Michael Smith, 72, stopped going to his doctor for a while and was rejected when he tried to return because the physician did not accept any new Medicare patients.
“He had his number, his quota for Medicare,” Smith said. “No matter how good of a patient you were, they don’t have to take it.”
Elko’s challenges exemplify how good benefits provided by mines can unintentionally damage the local health system. In addition to primary care challenges, expensive hospital bills, which some argue reflect the good wages and benefits the mines offer, have furthered inequities throughout the region and forced people to delay care or search for less expensive options hours away.
“Everybody here who’s been here awhile will say, ‘You know what, I will continue having my heart attack for three hours while I am in the car on the way to Salt Lake City rather than go to the [local] ER,’” said Brizee, the former state consumer health assistance ombudsman representing Elko.
The city of Elko sits toward the western edge of a sprawling, sagebrush-dappled county by the same name. The county is the size of Connecticut, Massachusetts and Rhode Island combined — with a population of more than 50,000. Residents assume driving hundreds of miles to Salt Lake City or Reno for specialty, or even primary, care comes with living in a rural area.
Only Elko has something many rural communities don’t: gold. The many mines in the region are a big reason that more than two-thirds of its population has employer-sponsored health insurance, one of the highest rates of any rural county, according to Census Bureau data.
Golden Health Family Medical Center siphons a significant chunk of those with good-paying mine insurance from the rest of the primary care community.
In most of the country, that would be the recipe for a stable health care infrastructure. But in Elko, the ample benefits offered by the mines creates a two-pronged problem. Golden Health, the clinic run by Nevada Gold Mines for its employees and their families, siphons a significant chunk of those with good-paying mine insurance from the rest of the primary care community. Physicians in private practice are left to fight over the remaining commercially-insured population — even though much of the need is from those on Medicaid and Medicare.
That makes it even harder for the community to recruit physicians to open a private practice, given Elko’s remoteness and rural workforce challenges. Elko has nearly half the number of primary care doctors per capita, two-thirds the number of dentists and a third the number of mental health providers compared with the national average, according to County Health Rankings.
“We should be able to have a really great health care system established, especially with the kind of benefits and the kind of income that a lot of the population in Elko are receiving,” said Dr. Bridget Martinez, who completed part of her medical residency in Elko. “There’s a huge deficit there that really doesn’t make any sense.”
‘That’s the sad part’
Elko’s health care landscape is fragmented.
More than 11,000 people in northeastern Nevada are employed by the mining industry. Two-thirds of them work either directly or as contractors for Nevada Gold Mines — a venture between former competitors Barrick and Newmont that operates the single largest gold-producing complex in the world.
While some miners are mistrustful of the Nevada Gold Mines clinic — likening it to company doctors of the past, known for caring more about the employer’s needs than the employees’ — it is a resource for those injured on the job who need to be treated and cleared to work.
In general, miners can expect to receive affordable primary care close to home and financial assistance to cover lodging and travel for out-of-town care, while their former coworker, just retired, will likely struggle to find quality, affordable care in the area.
“It’s good for the mine employees, but it takes away the primary care base for everybody else,” said Gerald Ackerman, assistant dean of rural health at the University of Nevada, Reno School of Medicine. “The challenge is it splits that health care.”
Nevada Gold Mines did not respond to requests for comment.
Some who don’t work at the mines use the local federally qualified health center, which receives federal subsidies so it can afford to take more patients with Medicare and Medicaid than a private doctor’s office. Others rely on urgent care clinics that offer primary care services. Still others must travel hours to Idaho, Utah or elsewhere for primary care. Some get so frustrated they give up.
“A lot of them are just fed up … and say, ‘I’m not even going to try anymore,’” said Sonia Ruiz, assistant director of the Medicare Assistance Program at the statewide nonprofit Access to Healthcare Network.
“There’s more people to be seen now than there are providers in town,” said Dr. Steven Lore.
Dr. Steven Lore, the only physician at the federally qualified health center, said he doesn’t want people traveling to Salt Lake or using urgent care for primary care needs. But he knows his facility, part of a chain called Nevada Health Centers, doesn’t have enough providers to meet demand.
“That’s the sad part,” Lore said. “There’s more people to be seen now than there are providers in town.”
People in Elko are equally, if not more, frustrated with their hospital.
Everybody here who’s been here awhile will say, ’You know what, I will continue having my heart attack for three hours while I am in the car on the way to Salt Lake City rather than go to the [local] ER.'
Jan Brizee, the former state consumer health assistance ombudsman representing Elko
The local, private equity-owned hospital, Northeastern Nevada Regional Hospital, has a bad reputation in the community for charging high prices — while being, at points over the last decade, one of the most profitable hospitals in the state. Residents feel an out-of-state company is profiting off them. The county health board, which includes all county commission members, once sent a letter to the hospital’s parent company complaining about the facility’s “anticompetitive pricing.” Brizee, who reviewed patient bills as a state ombudsman, said the hospital routinely charged far more than what people in Las Vegas paid for equivalent services, which she believes is a result of the good-paying mine wages and the hospital charging what it thought the community could afford. The median household income in Elko is roughly $82,000, nearly 30 percent more than it is in Las Vegas.
Hospital officials deny their charges have anything to do with miners’ salaries and argue it’s difficult to compare their bills to facilities’ in Las Vegas.
Hospital officials deny their charges have anything to do with miners’ salaries and argue it’s difficult to compare their bills to facilities’ in Las Vegas because of differences in the costs of labor, supplies and equipment, among other things. They also note that the hospital has worked with local elected officials and industry, including mining, to ensure the facility is meeting Elko’s needs and cite a number of ways the hospital supports the community, such as offering a free drive-through flu shot clinic and providing more than $20 million in charity and uncompensated care last year.
“As the only acute care hospital within a 125-mile radius, we believe that healthcare is delivered best close to home,” the hospital said in a statement. “[The hospital] regularly evaluates our rates and the services we provide and is committed to working collaboratively with payers, the mining companies, local healthcare providers, and all our community partners to ensure that everyone in our community has access to the care they need.”
Andrea Hasselhurst, chief nursing officer, gives a tour of the Elko Community Health Center. The outpatient surgery center could improve access to some specialty care in Elko.
‘It’s a problem’
These primary care and hospital challenges have their own ripple effects.
The mines and other large employers, looking to avoid the hospital’s high prices, have contracted with a surgery management company that coordinates out-of-town care, often in Salt Lake, to save money. Patients who have the means travel on their own.
Doctors argue this exacerbates the community’s specialist workforce shortage. With many of the best-insured patients traveling out of town, it’s harder to attract physicians who might give people a reason with good insurance to stay.
“Basically, that keeps out the possibility of some new gastroenterologist coming in and setting up his own shingle. ‘Well, wait, the paying portion of the procedures are now being sent to Salt Lake,’ so you’re left with just the Medicare and no one else,” said Dr. David Hogle, a private practice primary care doctor in Elko.
An out-of-state company that in March opened an outpatient surgery center in town could improve access to some specialty care. It accepts the insurance and surgery management plan offered by the mines, Medicare, and veterans and Indian Health Services benefits and eventually expects to take all plans, including Medicaid, according to Angela Browning, the center’s business office manager.
There’s a huge deficit there that really doesn’t make any sense.
Dr. Bridget Martinez, who completed part of her medical residency in Elko
Kevin Lutz, executive vice president of health care operations, policy and research at Community Health Development Partners, said the company chose Elko for its first surgery center because of the community’s needs and its high rate of commercial insurance. Lutz said people shouldn’t have to travel for care the community could support.
“The good thing about Elko, and probably most mining communities, is they have good benefits, and that could keep a business solvent,” Lutz said. “If you only took 80 percent Medicaid or Medicare, you couldn’t operate.”
Surgery center staff said they’re trying to recapture the population leaving town for surgeries, not compete with the hospital. But Ackerman, the assistant dean of rural health at the University of Nevada, Reno School of Medicine, worries that’s what could happen. For instance, if fewer people go to the hospital for outpatient cardiology, that’s less reason to keep around a cardiologist who could also provide emergency cardiac care — something the surgery center, by definition, cannot do.
“We will have an emergency in this community at some point in time, like we’ve had in the past where you have a mine bus accident or something like that, and then all of a sudden the services that you expect at your hospital to take care of your emergency aren’t there,” Ackerman said. “It’s a problem, and I don’t know what to do about it.”
Dr. Adam Stenseth (center), chief of staff at Mountainview Medical Center, said the hospital gets five or so serious medical calls — usually heart attack or stroke — a month.
Janie Osborne for POLITICO
PART 3: WHITE SULPHUR SPRINGS
A volunteer ambulance crew burst through the doors of the emergency room at Mountainview Medical Center just after noon on a late summer day. Staff surrounded the patient, who was having a heart attack. The emergency room was quiet save the staff’s low voices, a dripping faucet and beeping machines.
Dr. Adam Stenseth, the hospital’s chief of staff, ducked out from behind the curtains surrounding the patient’s bed.
“He’s pretty critical,” he said. “He might not make it.”
But Stenseth and the medical team stabilized the patient, and a helicopter transported him from their small hospital in White Sulphur Springs, Montana, 150 miles to Billings into the care of a cardiologist. The hospital gets five or so serious medical calls like this — usually heart attack or stroke — a month, Stenseth said.
An emergency helicopter from Billings Clinic prepares to transport a patient from Mountainview Medical Center to another facility. Mountainview receives additional federal funding because it is a critical access hospital, but it has had to fight to stay open.
Janie Osborne for POLITICO
“If we didn’t have the hospital here … really, in terms of trauma or stroke or any emergency situations, there would be a lot more people who wouldn’t make it,” he said.
Roughly 85 percent of the hospital’s patients have either Medicare or Medicaid, with commercial plans and uninsured patients making up the rest. The medical center receives additional federal funding because it is a critical access hospital, a designation for certain small, rural hospitals, but it has had to fight over the years to stay open. A local cattle rancher once put up his property as collateral to help the facility, and the hospital in recent years has operated on thin margins.
“It’s kind of like a person living paycheck to paycheck,” said Chris Schlepp, another rancher and hospital board member.
The opening of a copper mine 17 miles outside of town stands to change that, bringing good wages and robust health plans with low copays and deductibles to roughly 240 full-time employees and their families. Even if only half of those live in town, like the company estimates, that would mean significantly more commercial insurance and, by extension, a financial boost for Mountainview Medical Center.
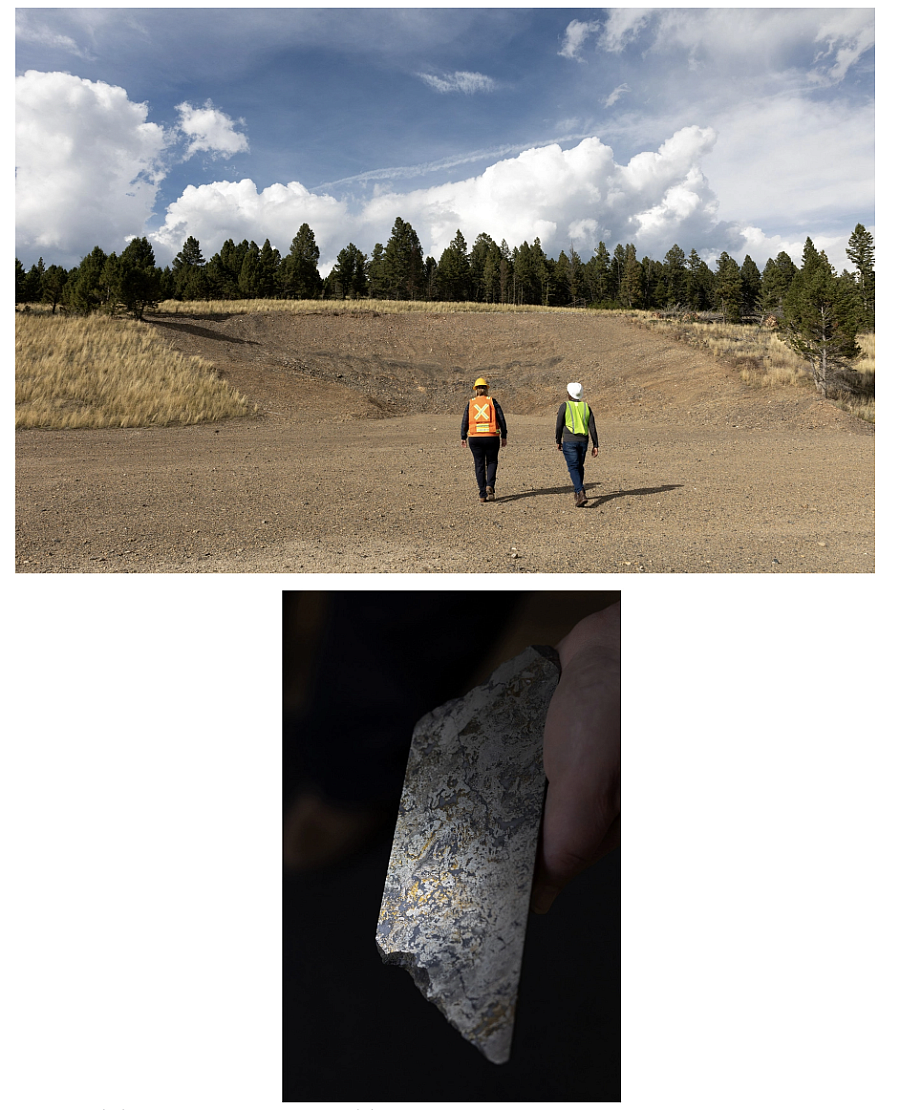
Top: Lincoln Greenidge (right), CEO of Sandfire Resources America, Inc., and Nancy Schlepp (left), the company's vice president of communications and government relations, walk toward the area that is the beginning of the future Black Butte Copper tunnel. Bottom: A sample of drill core that shows very high levels of copper is shown.
Janie Osborne for POLITICO
But the Black Butte mine could also hurt access, as happened in Elko or Williamson, if the hospital doesn’t plan carefully. It’s something hospital CEO Rob Brandt is already working to avoid.
“You [can] get complacent and start to spend that money that has a limited timeframe on an income stream, so to speak,” he said.
With the West on the verge of a mining boom to deliver on national priorities, the lessons of boomtowns past are top of mind in White Sulphur Springs. The copper rush hasn’t come yet to this tiny pocket of central Montana, and they’re already preparing for the day it goes bust.
“That’s the big thing. We’re all going to love and benefit while it’s here,” said White Sulphur Springs Mayor Rick Nelson. “The minute they close the doors and everything’s gone, what happens?”
Mountainview Medical Center is beloved by the community, which put up donations and purchased shares in the 1950s to finance construction.
Janie Osborne for POLITICO
‘Opening Pandora’s box’
Mountainview Medical Center, with its associated clinic, is the only place you can get medical care within 40 miles of this rural town nestled among three mountain ranges in central Montana. Those in the county’s outlying areas, like Ringling and Lennep, are farther from care.
Alaina Morrison, who owns a sporting goods store in town, said the hospital has saved her thousands of dollars in lost wages and gas. Without it, she would have to drive an hour or more to Livingston or Bozeman to manage a thyroid disorder that requires frequent blood draws and for doctor’s visits for her toddler.
“He has probably been to this doctor, to this hospital, six times since he’s been born,” Morrison said. “I’m so thankful that we have the hospital here.”
The hospital is beloved by the community, which put up donations and purchased shares in the 1950s to finance construction. But it’s grappling with the problems plaguing so many rural hospitals: an aging population with growing health care needs and little good-paying commercial insurance to cover the costs of care.
A much improved payer mix will help the hospital, though increased demand and overreliance on that good-paying insurance could strain it in the long run absent careful planning.
The bulk of construction at Black Butte has not started, but the hospital is already considering staff needs.
Rob Brandt believes it’s unlikely White Sulphur will see its health care grow and fragment the way Elko’s has because of the comparatively small number of people Black Butte will employ.
For instance, the mine is looking to partner with the hospital to bring health care to its site, which Brandt said would require hiring an additional provider. It’s also expected to increase overall health care demand, in the form of routine doctor’s visits for miners and their families and, likely, emergency medical care for mine-related injuries. Mountainview has two doctors and two physician assistants — who work in the hospital and the clinic — and Stenseth said the mine could put a significant burden on his team if it isn’t able to recruit one or two additional providers.
“It could be opening Pandora’s box because you don’t know what they’re coming in with,” Stenseth said. “If they generally don’t like to go to doctors — which lots of people don’t, they’re strong, rough and tough men and women who are just used to going for it — they may not come in until things are really bad, and that makes our job harder.”
Brandt, however, believes it’s unlikely White Sulphur will see its health care grow and fragment the way Elko’s has because of the comparatively small number of people Black Butte will employ.
“You can never say never,” he said, “but the numbers aren’t there to support another entity coming to open up a direct clinic for the mine.”
Details at Mountainview Medical Center, including a clinic sign (top left), medical supplies (top right) and a patient bed (bottom) are shown. The mine insurance could be a financial boon for the hospital as it expands.
Janie Osborne for POLITICO
The hospital broke ground in late September on a $42.5 million facility Brandt said will offer more medical services to the community. The goal, he said, is to save patients from traveling for their care and keep their medical spending at home.
The mine insurance could be a financial boon for the hospital as it expands, helping replenish its coffers, pay down its 30-year bond more quickly and allow for more services. But Brandt said that he is making his financial calculations independent of the mine’s plans so they’re not in a difficult position if those plans change.
“That was the promise that I had made to the board: With all the forecasts that we do, the mine is just gravy on top as far as increased patients in our community,” Brandt said.
White Sulphur Springs' fears echo the realities in Elko, where the high costs of not just hospital prices but rent and gas are common complaints among locals.
Janie Osborne for POLITICO
‘No one-size-fits-all solution’
It’s hard to disentangle the hospital’s fortune from that of the community.
There’s hope that the tax revenue from Black Butte will be a boon for the town, including helping it fix pothole-riddled streets and unearth sidewalks that have been paved over. But there’s also fear about the mine workers’ salaries driving up housing prices, already inflated by spillover demand from Bozeman and people from out of state seeking a slower pace of life.
“Just because there could be money here doesn’t mean we double the price of burgers and this and that because people can afford it,” said Nelson, White Sulphur Springs’ mayor. “We don’t want to jack rent up to $2,000 a month because the miners will rent when we’ve got people that have lived here their whole life, so to speak, paying $800 a month.”
The town’s fears echo the realities in Elko, where the high costs of not just hospital prices but rent and gas are common complaints among locals.
“We’re planning for the future, both on the environmental side, the economic side and the sustainability side," said Nancy Schlepp.
Janie Osborne for POLITICO
And a housing crunch could complicate the hospital’s efforts to recruit staff to meet increased demand for medical services. Brandt, a former hospital administrator at the edge of the Bakken, a region that covers parts of Montana and North Dakota, saw oil and gas workers flood the area and price out hospital staff. His old hospital at one point owned roughly a dozen housing units just to meet the needs of employees.
Mountainview is eyeing a public-private partnership to build homes next to its new hospital. If it can’t find housing for its workers, the hospital would be forced to lean more on traveling staff, which could drive up prices.
“The minute they close the doors and everything’s gone, what happens?”
Rick Nelson, White Sulphur Springs Mayor
The town is so mindful of the mine’s potential impacts that it’s formed an organization called the Meagher County Stewardship Council, which Brandt chairs, to negotiate a community benefits agreement. Its goal is to ensure the community takes advantage of the boom — the additional jobs and revenue — while also planning for the bust. Other communities — like Salmon, Idaho, where exploratory drilling for cobalt has started — are trying to develop similar agreements, which have traditionally been more common in Canada, Europe and Australia.
“Housing, health care, education — all of those pieces need to be in line so that when these people come in, we’re organized and we’re prepared,” said Cassie Coburn, the stewardship council’s executive director.
The mine, which employs several Meagher County natives in top positions, is collaborating with the stewardship council and the community. And mine leadership is hopeful that an influx of new people will help the hospital grow its patient base.
Including representatives from mining companies on local health boards and foundations could mitigate unintended consequences that good benefits have on the health infrastructure.
Janie Osborne for POLITICO
“We’re planning for the future, both on the environmental side, the economic side and the sustainability side. We’re already thinking about, ‘This is only here for a finite amount of time. Let’s make sure that we’re using this time wisely and doing things the right way,’” said Nancy Schlepp, a native who is vice president of communications and government relations for Sandfire Resources America, the company that will operate Black Butte.
Matt Vincent, executive director of the Montana Mining Association, said including representatives from mining companies on local health boards and foundations could mitigate unintended consequences that good benefits have on the health infrastructure.
“These relationships allow them to learn first-hand of any challenges,” Vincent said in an email. “Each community is different, as is each health care provider, mining company, benefits package, etc. There is no one-size-fits-all solution.”