
Beyond Shared Identity: Is an Indian Therapist Always the Right Fit for you?
This story was produced in partnership with India Currents for the USC Center for Health Journalism's Ethnic Media Collaborative.


The right therapist isn’t always someone who looks like you. Lavaanya’s story challenges the assumption that sharing ethnicity automatically means having common perspectives or an immediate sense of connection.
Polina Zimmerman
pexels.com/@polina-zimmerman/
In the early 1990s, Laavanya was the quintessential Indian American success story. The daughter of a physician, she grew up in New Jersey, an academic high achiever who went from a master’s in public health straight to medical school.
Yet alongside her intellectual brilliance, Laavanya experienced constant inner turmoil beginning at an early age.
Her father, a physician, recognized symptoms of depression and anxiety in his daughter and arranged for Laavanya to see an Indian-origin adolescent psychiatrist and a therapist who was not.
Propelled by a near-genius verbal IQ of 140, Laavanya excelled academically. But her verbal mastery masked her struggle with “subtle social issues,” such as difficulty interpreting body language and unwritten social norms.
“I couldn’t really read a room well or pick up on people’s vibes,” admits Laavanya. “I was always blunt. I never had filters.”
Though her medication was effective, the clinicians she saw — even the Indian psychiatrist her father found her — did not identify her neurodivergence or fully grasp the nuances of her “bicultural identity” as an Indian American.
“Those years just seemed like such a blur to be honest,” says Laavanya, reflecting on a mental health journey that began in her teens and took years to get clarity on her conditions.
“Remember, this was the early ‘90s,” explains Laavanya. “The only psychologists that were available were white.” Issues like immigrant parents, children juggling two cultures, assimilation versus acculturation, and multicultural psychology were not issues the field of psychology was addressing yet.
In 2003, while at medical school, Laavanya was diagnosed with mild Asperger’s syndrome at age 27 after numerous neuropsychological evaluations. The social, emotional, and physical pressures reached a breaking point during an internship, and Laavanya dropped out of medical school. “I realized I wasn’t really cut out to be a physician or to practice clinically.”
Had she had a diagnosis earlier, says Laavanya, she’d have “looked into other nonclinical areas of health care” for a career. She eventually trained as a biometric screener and became an advocate for mental health.
Lavaanya’s story challenges the assumption that sharing ethnicity automatically means having common perspectives or an immediate sense of connection. She found that working with a South Asian American therapist did not necessarily mean the therapist was the right fit. Identity is shaped by much more than race or culture, and each person’s path to healing is unique.
Treating immigrants also poses a unique challenge for mental health practitioners in the U.S. When first-generation immigrants, American-born children of immigrants, and people navigating multiple cultural identities have very different needs, how do clinicians provide care that reflects the diverse realities of immigrants, and what does it really mean for mental health care to be culturally congruent?
A Generational Culture Gap
Laavanya’s story is unusual in that her family was always supportive of her mental health journey, unlike many Indian households, which do not discuss mental health openly.
She says but the “culture gap and generation gap” in her home environment contributed to her struggles.
“I was part of the first generation being raised here by the immigrants that came in the ‘60s and ‘70s. It was a very different time.”
As her parents tackled the pressures of adapting to a new culture and establishing their lives from scratch, their children faced a different set of challenges, growing up between two worlds. Second-generation South Asians like Laavanya often live one life at home, steeped in Indian culture, and another outside, which is more American.
While her first therapist talked about symptom management and how she felt participating in everyday life from hobbies to exercise, there was no discussion about “issues of parenting and identity formation, cultural conflict and emotional awareness,” says Laavanya.
Roots of her Dual Identity
Growing up, Laavanya felt a stronger connection to American culture, explaining that she “got along much better with mainstream Americans” than with other South Asians, objecting to what she perceived as the excessive focus on wealth and achievement as “showy and shallow.”
Despite disconnection with fellow desis, Laavanya loves Indian culture, especially its “intellectual richness and humanism,” which her father taught her to value.
She has traveled across India, discovering her Indian heritage, learning about its “languages, classical art forms, spirituality, history, traditions, rituals, clothes, food and more. I feel Indian culture is this incredible treasure in which one can learn endlessly for a lifetime.”
In 2020, Laavanya finally had a breakthrough. She met an Ecuadorian American immigrant therapist with expertise working with high-functioning neurodivergent patients. The therapist used a trauma-informed, culturally sensitive approach that helped Laavanya connect her bicultural identity with her neurodivergent brain.
“I thought since I was very Americanized and assimilated that I didn’t need to address these bicultural issues,” says Laavanya, but “through her I realized that even if I never really got along or felt at ease or at home with Indians or my own community, the cultural duality will always be there.”
“I’m still the brown woman in white spaces.”
When Shared Identity is Not Enough or Not Preferred
Identity is complicated for South Asians in America, says Dr. Hari Nair, a Child, Adolescent and Adult Psychiatrist, who sees many South Asians at his Bay Area practice. A first-generation immigrant may have very different needs from someone born and raised in the United States.
“I’m sensitive to the fact that some Indian patients want a non-Indian therapist because they want a 'blank canvas.'” — Dr. Hari Nair
Patients often come to him because he shares their cultural background, so Dr. Nair looks for points of connection to build trust. “It’s cultural things like home cooking or going to the temple. My parents, who came from India in ’77, always preferred Indian doctors because of that connection. You want to feel comfortable when talking about difficult things.”
While matching patients with therapists who share their ethnicity is believed to boost cultural competence, Dr. Nair is careful not to assume that a shared background equates to a shared experience.
“I guard against the idea that because we’re both Indian, I know exactly what they’re going through,” says Dr. Nair, acknowledging that being Indian just gets his foot in the door. “Then I have to be curious about their specific life.”
Conversely, some South Asian patients actively avoid providers from their own community to escape perceived social or cultural stigmas. “I’m sensitive to the fact that some Indian patients want a non-Indian therapist because they want a ‘blank canvas’” without the perceived judgment of their own culture,” adds Dr. Nair.
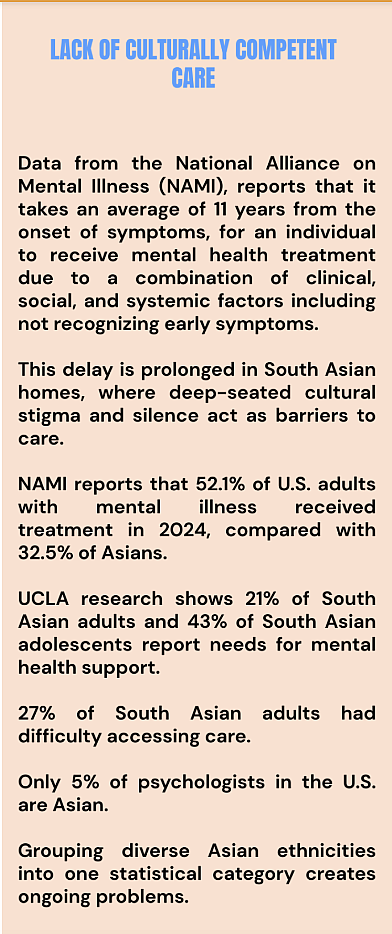
The National Alliance on Mental Illness (NAMI) reports that on average, people wait 11 years from the onset of symptoms before receiving treatment.
In South Asian families, cultural stigma and silence can make that wait even longer.
Although more than half of U.S. adults with mental illness receive treatment, only one-third of Asians do. Many South Asians report needing mental health support but struggle to access care, a problem made worse by the shortage of Asian psychologists and by the grouping diverse Asian communities into a single statistical category.
A Breakthrough Diagnosis
With her therapist, Laavanya developed a better understanding of her neurodivergence and how to address the intergenerational trauma that came from her Indian background. She learned to acknowledge “the unrealistic expectations that success means only attending elite universities and having prestigious jobs in specific fields. I’ve had to redefine success in other ways.”
In December 2023, her therapist recommended another neuropsychological evaluation. Laavanya says she was diagnosed with “high-functioning autism and nonverbal learning disability(NVLD).”
While no two people with autism have the same symptoms, high-functioning autism is used to describe a person who may thrive academically but exhibit a delay or lack of social skills. They can have difficulty understanding the feelings and reactions of others, which can make them appear to be insensitive at times.
Not widely understood or known, NVLD is characterized by challenges with visual-spatial reasoning and interpreting nonverbal social cues, while verbal abilities are often relatively strong.
Why did Laavanya’s diagnoses take so long? In her case, what was missing was the right combination of clinical expertise and cultural understanding needed to recognize her particular set of conditions. Seeking care from an Indian-origin clinician was not, by itself, the solution.
When Your Mental Health Provider Gets You
For a creative and driven Bay Area teenager, Kiana’s (name changed for privacy) path to therapy began when she realized that despite working twice as hard as her peers, she still wasn’t achieving the academic results she wanted.
An only child in a South Asian family, Kiana loves to dance and is passionate about community service. But she is all too familiar with “cutthroat” academic competition and the cultural pressures to “strive for perfection” that often define her environment.
Her world is very different from the one Laavanya experienced as a teen. Today, the Bay Area is a thriving hub for Indian Americans, making it less likely for young people to feel different because of their cultural background.
With her parents’ support, Kiana sought treatment for school-related anxiety and overstimulation. She says working with an Indian-American psychiatrist has been transformative because of their shared cultural background.
“It helps me to have someone to relate to and have someone that understands the same cultural context,” Kiana says. Her psychiatrist understands the academic pressures children encounter in South Asian communities, which “can be really intense …there’s a lot of high achievers and a lot of people that outperform others,” reflects Kiana. Her psychiatrist’s firsthand understanding of the Bay Area’s culture of high achievement helps guide young people like Kiana, many of whom “feel like they’re not doing enough.”
After a neuropsychological exam in her sophomore year, Kiana was diagnosed with Generalized Anxiety Disorder; a second exam in her junior year resulted in a definitive diagnosis of mild Non-Verbal Learning Disability (NVLD).
Her diagnosis and a strong relationship with her psychiatrist helped Kiana manage her anxiety and learning disability through talk therapy and dialectical behavior therapy (DBT), while coping with the intense academic pressures of high school.
She attributes the value of her therapy to her psychiatrist’s cultural understanding of “ how my parents communicate and how that kind of differs from an American household.”
Dr. Nair, who grew up in the U.S., relates to the challenges his young South Asian patients face. “Academic pressure, balancing STEM with the arts, the expectation to become a doctor — I get it,” he says.
That shared perspective helps him better understand their experiences navigating cultural and generational differences within their families and communities.
Finding Her Fit
At almost 50, Laavanya has also been a mental health advocate for 5 years. She wants to share the insights she gained from her complex mental health journey to help others navigate a path that is often challenging.
She was recently nominated for the 2026 NAMI NJ ‘In Our Own Voice’ Award.
Life is a process of self-discovery, Lavaanya says. “I think one of the crucial things that I found out about when I was doing mental health advocacy work with South Asian mental health is just because you’re a U.S.-raised South Asian-American doesn’t necessarily mean that you are equipped to work with our community in this space.”
Laavanya continues to live at home with her parents, where she feels very lucky to be loved and supported.
She is more at peace with herself. “I just want to be me. I’m not willing anymore to remold myself to fit into a neurotypical world.”