
Mothers Face Broken Addiction Treatment System
The story was originally published in MedPage Today with the support from USC Annenberg Center for Health Journalism’s 2022 Data Fellowship.

Kayla Quinones began having contractions a few hours after midnight. Her baby, Jacarri, was on the way.
Quinones, 33, was homeless at the time and staying with a friend in upstate New York, and when she began to feel the undulating pains, spaced about 8 minutes apart, she called for help. Those pains, her friend told her, were contractions. They needed to get to a hospital.
Before staying with her friend, Quinones spent 6 years living on the streets of Sullivan County, about 2 hours north of New York City. She had been using heroin for 7 years, and cocaine for the last 4. She was homeless for the majority of her pregnancy. And using for all of it.
Doctors rushed Quinones to the delivery room, and the birth went smoothly. Jacarri was born healthy, but had developed neonatal abstinence syndrome. At the time of his birth, Jacarri had methadone and cocaine in his system, so doctors transferred him to the neonatal intensive care unit at a nearby hospital. The hospital where Quinones delivered him did not have one.
After Jacarri's birth, Quinones was more motivated to get help for addiction than ever before. Jacarri's father, Quinones' longtime partner, died when Quinones was 4 months pregnant, and she was now learning that she'd lost custody of her baby. Jacarri would be going to stay with Quinones' mother in Queens and would stay there until Quinones could get into a treatment program. She was again living on the street, searching for a program that would take her in.
It wasn't the first time she had looked for help. She had been enrolled in a methadone program during her pregnancy, but continued to use heroin.
Now looking for a more comprehensive treatment program, Quinones ran into a new problem. Because she hadn't received a postpartum check-up -- which typically occurs between 4 and 6 weeks after delivery -- many treatment centers wouldn't take her, she said.
"They were denying me left and right," Quinones told MedPage Today. "I was still running the streets, and miserable because they took my kid away. And I was worried that I wasn't going to get into a program."
In an underfunded, siloed mental healthcare system, pregnant and postpartum people with addiction face endless barriers to treatment. While patients typically come into contact with the medical system more frequently during pregnancy, those with addiction struggle to get adequate care, as insufficient numbers of behavioral health providers, logistical hurdles, and distrust of the medical system deter people from accessing treatment, according to providers, patients, and advocates.
"There is a presence of substance use that often gets overlooked and undertreated in pregnancy," said Leah Habersham, MD, an addiction medicine specialist and ob/gyn at Mount Sinai Health System in New York.
Medication-assisted treatment (MAT), such as buprenorphine (Suboxone) and methadone, are the gold-standard treatment for pregnant patients with substance use disorder. These therapies manage cravings and prevent patients from going into withdrawal, which can result in preterm delivery or fetal growth issues.
But not all patients can access MAT, data show. Nationally, only half of pregnant patients with opioid-related substance use who received care at an addiction treatment center received methadone treatment in 2020, according to an analysis performed by MedPage Today.
Those who seek treatment in New York, where Quinones lives, receive it at a rate higher than the national average. In 2020, there were 635 episodes of treatment involving opioid use in pregnancy at New York addiction treatment centers. Of those treatment episodes, 75% received MAT at discharge.
The data, which come from the Substance Abuse and Mental Health Services Administration's (SAMHSA) treatment episodes database, is a compilation of addiction treatment center data reported by state agencies. Many of the treatment centers that report to SAMHSA receive state funds or federal block grants to provide drug or alcohol treatment services, the agency says.
Of the 6,200 times pregnant patients received opioid-related treatment nationwide in 2020, all received care at addiction treatment centers, such as methadone clinics or specialty behavioral health centers. However, providers say this is an underestimate of patients that receive care.
Many patients access treatment for substance use disorder outside of specialty care facilities, including from a family medicine provider, addiction specialist, or ob/gyn practitioner who prescribes buprenorphine -- treatment that is not recorded in public databases.
Not knowing how many patients do or do not get treatment poses a host of issues, according to patients, providers, and advocates. Without an accurate count, it's difficult to properly allocate resources to treat substance use disorder among the population of pregnant patients, they say.
"We don't know how many people receive comprehensive services," said Mishka Terplan, MD, MPH, a board-certified ob/gyn and addiction medicine specialist based in Maryland. "And that's really kind of unknowable."
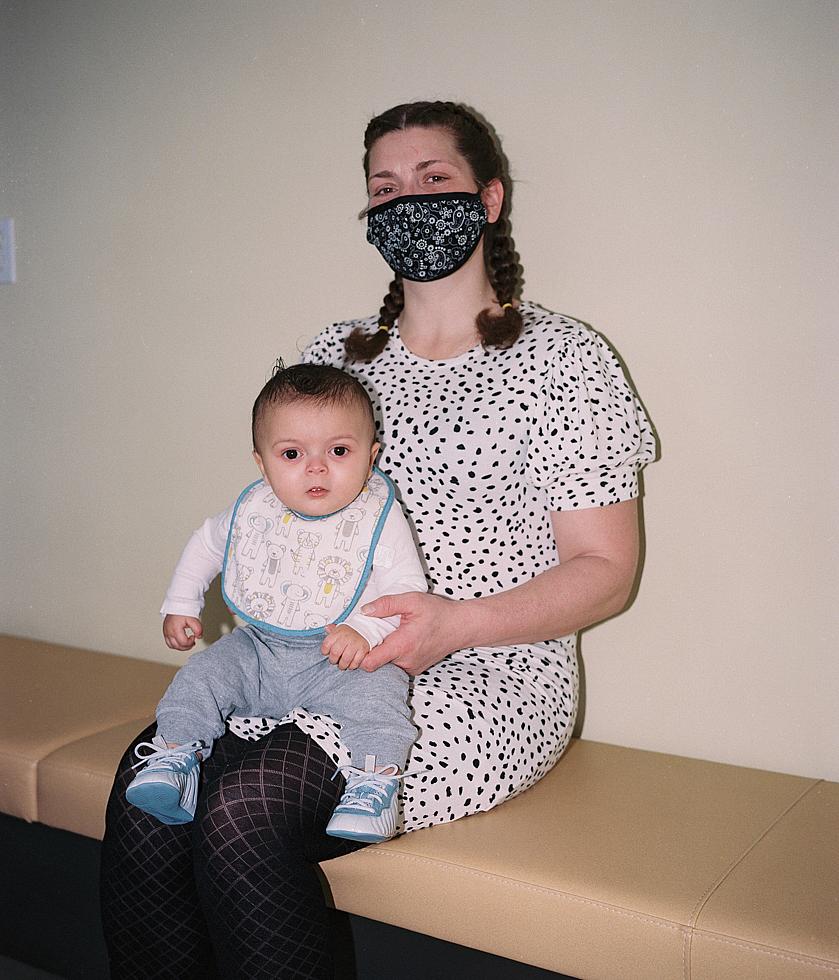
Kayla Quinones, who lives with her son Jacarri at Greenhope Services for Women in East Harlem, New York, looked for treatment centers for a month before enrolling in the residential treatment program at Greenhope. Before having her baby, judgment and stigma from medical providers prevented her from seeking care, she says.
Photo by Liam Quigley.
A Growing Problem
More than 1 million peopleopens in a new tab or window have died of an overdose since the opioid epidemic began in the late 1990s. The crisis intensified during the COVID-19 pandemic, as isolation and interruptions to medical care led to skyrocketing overdose deaths.
Nationwide, there were an estimated 108,000 overdose deaths in 2021 -- an all-time high, CDC data showopens in a new tab or window. The majority of those deaths involved fentanyl, a synthetic opioid that's 50 times more potent than heroin.
Opioid use disorder trends among pregnant patients are directly connected to patterns in the general population, Terplan said.
In total, 6,000 women had a maternal opioid-related diagnosis at delivery in 2017, the most recent year for which data are available, according to a study in JAMAopens in a new tab or window. Self-reported data from the CDCopens in a new tab or window suggest that 6.6% of women used prescription opioids during pregnancy. One in five women who used prescription opioids reported misuse, the study showed.
"We all know that opioid use disorder is a rising problem, and it's hitting the pregnant population as well," said Wendy Wilcox, MD, chief women's health services officer at NYC Health + Hospitals, New York City's public hospital system.
The vast number of opioid-related deaths has left policymakers scrambling to solve a worsening addiction problem. Last October, the Biden administration released a planopens in a new tab or window to improve access to substance use disorder treatment for pregnant and postpartum people specifically.
The plan aimed to correct issues that were preventing patients from accessing MAT and looked to improve public reporting of access data.
Currently, there are no public databases that clearly show how many patients -- pregnant or not -- get medical treatment for substance use disorder. (Click here for moreopens in a new tab or window on the challenges of reporting data around substance use in pregnancy.)
Late last year, the federal government also deregulated buprenorphine to improve treatment access. Providers previously needed an X waiver -- a special Drug Enforcement Administration (DEA) certification -- to prescribe buprenorphine, which required an 8-hour training and restricted the number of patients a clinician could treat.
After years of rolling back restrictions, the federal government eliminated the X waiver entirelyopens in a new tab or window in December. The nixing of the rule allows any provider with a DEA license to administer buprenorphine, pending a one-time training.
Most ob/gyns are licensed by the DEA to prescribe controlled substances. But addiction medicine experts worry that though federal regulations on treatments for substance use disorder have begun to ease, there will remain a gap between the number of primary care providers and ob/gyns willing to prescribe buprenorphine and the number of patients who need it.
Should Ob/Gyns Provide More Addiction Care?
Medical organizations, including the American College of Obstetricians and Gynecologists (ACOG) and the American Society of Addiction Medicine (ASAM), have firmly said that they believe MAT is the gold-standard treatment for pregnant patients addicted to opioids.
Though there are three drug treatments available to all patients with opioid use disorder, methadone and buprenorphine are the most commonly prescribed treatments for pregnant patients. The opioid antagonist naltrexone (Vivitrol) is also safe to use in pregnancy, but is recommended less often because it requires patients to stop using opioids for about 2 weeks prior to initiating treatment.
Despite the recognition that MAT is widely believed to be the optimal treatment for opioid-addicted patients, providers who are not trained in addiction medicine still don't feel comfortable administering it, said Daniel Rosa, MD, medical director of the Acacia Network, a human services organization in the Bronx that provides addiction treatment services.
"The problem has always been the buy-in from ob/gyns and primary care providers," Rosa said. "It still falls on the very few people who happen to be board-certified in addiction medicine."
Methadone can only be dispensed through a SAMHSA-authorized opioid treatment program. But now, most ob/gyns and nurse midwives can prescribe buprenorphine, as long as they have a DEA license.
Before buprenorphine was deregulated, ob/gyns did not get certified to prescribe it in large numbers. Less than 2% of ob/gyns who treat patients on Medicaid had an X waiver as recently as 2019, according to a study in opens in a new tab or windowJAMA Network Openopens in a new tab or window.
"That to me, is evidence that the workforce has failed," Terplan said.
Addiction medicine is typically viewed as separate from reproductive healthcare, Terplan explained.
"Ob/gyns provide episodic care, and addiction is a chronic condition," Terplan said. "That's a clinical mismatch."
Even then, asking ob/gyns to initiate care for patients with opioid use disorder puts the onus on the doctors to treat the highest acuity patients in a different specialty, Terplan added.
Take treating a patient with diabetes, Terplan said. "The first time you take care of somebody with diabetes is not the person who's in a diabetic coma with a gangrenous foot in the emergency room. It's somebody in the outpatient setting who's on insulin, who brings their sugars, and you look at the sugars and you slightly adjust the insulin dose," he said.
"Basically, we've been asking people for the last 20 years to take up a new domain of health and start with the sickest patient. And, there's some DEA surveillance for the prescribing practices," Terplan said. "I don't think it's a categorical surprise that uptake has not been what it could be."
Until there is more training around the prescription of buprenorphine, experts are skeptical that the elimination of the X waiver alone will lead more ob/gyns and primary care providers to treat pregnant patients with opioid use disorder.
"I don't think it's going to be that ... a ton more primary care doctors or ob/gyns are going to start prescribing," said Amy Van Milligan, MD, an internist and pediatrician who provides MAT in Cincinnati.
Elimination of the X waiver takes away the mandatory 8-hour requirement, Van Milligan added, "but it's not going to make people magically comfortable with substance use disorder."
Why Treatment 'Just Doesn't Work' for Pregnant People
Just as some ob/gyns and primary care providers may have difficulty treating pregnant patients with opioid use disorder, providers comfortable with treating patients with substance abuse may not feel comfortable treating pregnant patients. It all amounts to a siloed system that some say makes it difficult to connect patients with the various types of care they need.
"There's still some confusion out there amongst MAT providers about how to care for pregnant people," said Jaine Fairbairn, a wellness coordinator at the neonatal abstinence program at Margaretville Hospital in New York. "And trying to find an ob/gyn who is versed on the actual prescribing of MAT is very difficult."
But once pregnant patients get linked to prenatal care and find an addiction treatment specialist, then the hard work begins: obtaining care.
Fairbairn works with around 10 pregnant patients at any given time. In addition to advocating for her clients in the exam room, Fairbairn connects her patients with resources like diapers or baby food, answers questions about what to expect at each stage of the baby's development, and helps patients coordinate transportation to medical appointments, she said.
In Delaware County, where Fairbairn works, the sheer logistics of getting to and from doctor's visits is one of the biggest challenges that patients face. The county is the size of the state of Rhode Island, but is home to around 45,000 people, she said.
"Here in the rural universe, methadone is almost impossible to maintain," Fairbairn said. "These places are all an hour, an hour and a half, two hours from wherever you are."
Medicaid transportation is available, but unreliable, Fairbairn added.
"Once a patient has been burned a couple of times, they just refuse," she said.
Child care and other family responsibilities also pose barriers. "Addiction treatment isn't easy if you have other kids at home," Van Milligan said.
During pregnancy, patients are already overwhelmed with the number of appointments they need to make with their ob/gyn alone, she said. Factoring in a different provider that administers MAT, coordinating transportation, and figuring out who is going to watch the kids at home -- it becomes nearly impossible for some patients to get treatment, she added.
"It's not that they don't want it, it just doesn't work," Van Milligan said.
In addition to the barriers to treatment posed by coordinating care, many pregnant patients with addiction may avoid treatment -- both for prenatal and addiction care -- because they don't trust medical providers.
Quinones first went to an ob/gyn when she was about 8 weeks into her pregnancy.
"I was nervous at first, walking in and knowing that I was going to have to tell him that I was an IV user," she said. On top of that, she used cocaine, had hepatitis C, and hadn't been to a gynecologist in 5 years.
"The doctor basically told me I was a junkie and I had to stop using, otherwise I wasn't going to be a good parent and my kid was going to come out just like me," Quinones said. At one point during the appointment, her physician told her it was still early, and asked if she was certain she wanted to keep her baby, she told MedPage Today.
Quinones walked out of the healthcare facility before even putting on a hospital gown. She didn't try to get prenatal care for the remainder of her pregnancy.
"I was disappointed, but already kind of knew that that was going to happen," Quinones said. "Because I've been through it so many different times."
While the stigma of addiction is enough to keep patients out of the doctor's office, they also run the risk of losing custody of their child or children. (Click here for moreopens in a new tab or window on the relationship between access to treatment and the child welfare system.)
Fear of the medical system and child protective services (CPS) prevents patients from telling their providers the truth about their substance use, Habersham said. Fear and stigma not only impact a patient's ability to get timely care -- it affects the public health system's ability to assess how many people may struggle with addiction in pregnancy.
Recently, Habersham saw a pregnant patient at Mount Sinai's female-only methadone clinic in New York City. The patient became addicted to prescription opioids, and then heroin, and was now seeking addiction treatment before going to the ob/gyn for prenatal care.
Habersham encouraged the patient to come to a clinic she started at Mount Sinai last year called the Bridge Program, which provides integrated addiction and reproductive healthcare. She told the patient that she could get her an ultrasound and labs so that they could begin to assess her pregnancy and initiate prenatal care. But on the day of her appointment, the patient was a no-show.
"She ended up not coming," Habersham said. Habersham reached out to the patient's social worker, who told her that the patient was fearful that her children at home would be taken away from her.
"I think that as we change the narrative, as we decrease the stigma, and as we start linking patients with treatment instead of linking them with CPS, that we are going to see the true numbers," Habersham said. "I don't think that in the current climate, that we're going to reach that point."

Greenhope Services for Women in East Harlem, New York, which is an affiliate of the Acacia Network, provides residential recovery services to women and their children. Children up to age 5 are eligible to stay with their mothers in treatment.
Photo by Liam Quigley.
The Push for Comprehensive Care
Habersham wishes there were more centers in New York for patients to receive a range of services at once -- prenatal care, behavioral health counseling, addiction treatment, and more.
In 2016, David Garry, DO, a maternal-fetal medicine specialist at Stony Brook Medicine in New York, started the Maternal Opioid Management Support (MOMS) program. The outpatient clinic provides buprenorphine treatment, behavioral health counseling, social services, and prenatal care.
"I think medication alone is not the answer, and I think that counseling alone is not the answer," Garry said. While medications can address the biochemical mechanisms in the brain that cause drug cravings, counseling helps patients work through mental trauma, he said.
Comprehensive care sites like the MOMS program exist throughout New York State, "but it's tricky to get them paid for," Terplan said.
Prenatal care is bundled, so it's often reimbursed to providers as one lump sum per pregnancy. When an individual provider gets a bundled payment for prenatal services, it can be seen as double-dipping when they charge fee-for-service payments for addiction care on top of that, Terplan added.
"It makes this integrated care by the same provider really difficult to realize," he said.
Some providers, like Garry, have gotten around that barrier. His program's ability to provide prenatal and addiction treatment in one place is not only cost-effective for patients, but it also reduces the stigma of accessing addiction care.
"They are just like any other patient in the office," he said.
Garry said that his clinic tries to follow up with patients 1 to 2 weeks after birth -- the postpartum period is a time when many patients may fall back into drug use. More intervention during this period could reduce preventable deaths, he added.
Almost a month after Jacarri was born, Quinones found a treatment center that would take her in, despite the fact that she had not received a postpartum check-up. She became enrolled at Greenhope Services for Women, a residential, female-only addiction treatment center in East Harlem.
Greenhope, a part of the Acacia Network, allows children up to age 5 years to stay with their parents in treatment. A month after Quinones arrived at Greenhope, a judge granted her custody of her baby. Jacarri, now age 7 months, lives with Quinones full-time.
Quinones has access to primary, pediatric, and addiction care through Greenhope's network of providers. She leaves the facility's campus for methadone treatment, and is steadily decreasing her dose of the treatment until she can wean off of it entirely.
The death of Jacarri's father, her fears for the future of her child, her unstable living situation -- it all served as a pull into addiction, while simultaneously motivating her recovery.
"Every reason why I was using was pretty much a great choice for it," she said. "But at the same time, everybody was also dying. I didn't want Jacarri to grow up without his mom."
But all the contradictions of addiction and every barrier to treatment were trumped by Jacarri, the boy who unknowingly provided the final push his mother needed to get care.
"He literally saved my life," she said.