
‘Is this what a good mother looks like?’
This article was produced with assistance from the USC Annenberg Center for Health Journalism’s Data Fellowship.
Other stories include:
An autistic teen needed mental health help. He spent weeks in an ER instead.
An autistic teen needed mental health help. He spent weeks in an ER instead.


Lisa Rowe at her home in Hendersonville, N.C. For years, she has struggled to get her son help in battles with insurance companies, school districts and treatment centers.
(Matt McClain/The Washington Post)
It was during his most recent outburst in January that she finally made up her mind — sometime between the moment he lunged for their knife drawer and when she dialed 911 for the 14th time in less than a year.
The police, as usual, took her son to the emergency room. But this time, when the hospital asked her to pick him up because they couldn’t find room for him at a psychiatric facility, she refused.
Now Lisa was preparing to explain her decision to a judge. After years of trying to obtain mental help for her child, she believed the only way to do it was to no longer be his mother.
To get him into a full-time residential treatment program and find a way to pay for it, she was willing to give up her parental rights. She would hand her son over to social services and open herself to charges of being a negligent parent. It was an act of desperation for Lisa — one that’s made by thousands of families across the country every year in the face of inadequate, inaccessible mental health care.
“I’m not a monster,” she told herself as she got out of her car and smoothed the soft pink blazer she had picked out that morning. “I love him. I’ve tried everything.”
Inside the small second-floor courtroom, a clerk handed Lisa a legal summons and told her to wait for the judge to call her name.
“I’m not a monster. I love him. I’ve tried everything.” — Lisa Rowe
“NEGLECT,” read the summons in her hand. “The mother is unable or unwilling to provide a safe home for the juvenile, or to comply with mental health recommendations.”
Lisa, 60, thought about the years she had spent battling insurance companies, hospitals, school districts and treatment facilities. She thought about her panic when her son first became suicidal at age 10. She thought about the coronavirus pandemic and how much worse things had gotten over the past two years: six trips to the hospital. Back-to-back alcohol and prescription pill overdoses. Clashes with authorities that inevitably ended with her son on the run.
“The juvenile has hit and spit on law enforcement officers. He has made threats to kill others,” the summons read. “The mother reports having to put her dresser in front of the door to prevent the juvenile from gaining access to her.”
She flipped the papers face down on the seat beside her so others waiting in court couldn’t see.
She worried what colleagues would think at her part-time job as a school psychologist, where she advised others how to help struggling children. She worried what the judge would say and how much she would be allowed to be part of her son’s life once the hearing was over. Most of all she worried how her son — whom The Washington Post is not identifying because he is a minor — would react.
He had called her the night before. She put him on speaker phone and tried to keep their conversation light.
“Hey, buddy, how you doing?” she said.
“Just chilling,” he answered.
After Lisa refused to retrieve him from the hospital, a case worker had her son sleep overnight at the social services office before assigning him to a temporary foster family.
“What’d you do at the social services office?”
“Just sat there.”
“I’m sorry. I wish it wasn’t like this. I really do,” Lisa said.
Her son answered her with silence.
“You know where they’re going to send you tomorrow?” she asked.
“No. If I ask too much, they might think I’m gonna to run again,” the teen said with a laugh. “Just kidding.”
“Thank you for saying, ‘Just kidding,’ ” Lisa replied. A few breaths later, she added quietly, “You’re not going to, are you? Please don’t.”
Lisa told him she had to go to bed so she could get up early for the court hearing. She didn’t know that in a few hours a call from police would interrupt her sleep — another crisis like so many before.
“You and I have been through hell together,” she told her son, as she prepared to hang up. “I love you, buddy.”
He had stopped telling her he loved her a while ago. But now, she thought she heard something like affection again in his voice. And it was causing her to second-guess so many of the choices she had made that week.
“Wait,” her son said over the phone. “Don’t leave yet.”

The boy she loved
In a small cardboard box, Lisa kept a picture of her first days holding him as a baby, her fingers enveloping his delicate newborn hands.
Lisa and her husband, who are now divorced, had been trying to have a second child for more than a year. Just days after Lisa miscarried, her sister, a police officer, told them about a heartbreaking case she had encountered.
A man had just walked out on his pregnant partner and threatened not to return unless she got an abortion or gave away the baby.
Within weeks, Lisa and her husband had secured a crib, a bigger car and a bank loan for $45,000 in adoption legal fees. The social worker vetting them as potential parents, Lisa recalled, asked whether her feelings might change if the boy was born with a disability like Down syndrome.
No, Lisa said she replied.
“You love them no matter what,” she remembers telling the social worker. “Once they become your child, you can’t imagine life without them.”
The baby was born with a heart murmur and spent his first days in intensive care. Lisa took lactation classes, determined as an adoptive mother to provide her son with breastmilk. In the years that followed, she would often recall the sweetness of those first weeks when she cradled his tiny body next to hers.
Those memories sustained her. She kept photos of her son’s best days scattered throughout her home. His face covered in chocolate at 3. Posing with Spider-Man during a family trip to Universal Studios.

She often slept with her favorite one under her pillow — her son at 7 after a day on the lake, his tousled hair framing the beginnings of a smile.
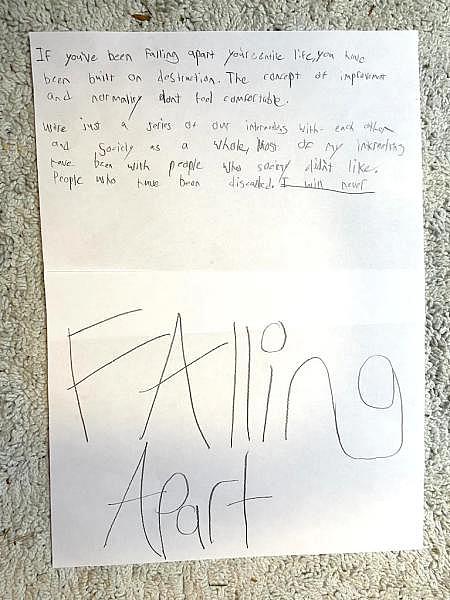
She also held onto reminders of the whip-smart teen he had become. His books on Buddhism and documentaries on minimalism. The pensive songs he wrote about the turmoil he felt inside.
“Guess it’s time to say goodbye to the dark, the scary dark. Where’s the switch? (I want the switch),” read lyrics he’d left on the dresser of his empty room just days earlier, before police took him to the hospital. “Red is mad, blue is sad. Pink is fun, yellow numb.”
On her laptop were screenshots of handwritten letters he’d sent to her at 15 while attending a 70-day survival program for teens struggling with addiction and mental illness.
In the wilderness, he described the fireflies and stars he was seeing at night. “The vast distances between towns gives oneself a sense of awe,” he said. He talked about his hopes for college and living out West.
“I really do miss you,” he wrote his mom. “I love you to the andromeda galaxy and back.”

The spiral into darkness
The screaming tantrums began at 3. Then came developmental delays, repetitive tics. He threw chairs in elementary school and bit his own arms until he bled.
With each specialist they saw came a new diagnosis: neurosensory issues, depression, anxiety, autism, Tourette’s, attention deficit and hyperactivity, disruptive mood dysregulation, bipolar, oppositional and obsessive-compulsive disorders.
A long list of medications was prescribed: Zoloft, clonidine, Adderall, prazosin, Abilify, lithium, Lamictal, Vistaril, Cymbalta, Zyprexa, trazodone.
By the time he was 10, he was talking constantly about killing himself.
After his most serious suicidal episode in 2014 — when he made plans to climb a 200-foot-high tower and jump — Lisa found herself camped out for three months at the hospital while he waited for psychiatric treatment.
There were never enough psychiatric beds, especially for kids. A charity, the Ronald McDonald House, gave her a place to sleep near the hospital. But surrounded by other families battling cancer and other physical diseases, she felt like an outcast.
“No one blames a kid for getting cancer. No one blames their parents,” she said. “But people just don’t think of mental illness like that.”
They were living at the time in a rural town in New Mexico. The few mental health services Lisa was able to find — three hours away in Albuquerque — were often restricted by Medicaid and the insurance company, UnitedHealthcare, that managed her son’s Medicaid-funded treatment. The insurance company was willing to authorize payments for trips to the ER whenever her child struggled with suicidal impulses, but it balked at many of the full-time residential treatment options for which Lisa pleaded.
UnitedHealthcare declined to answer questions about the case, but said in a written statement: “We are committed to supporting our members through access to quality mental health care. Over the last several years, we have taken concrete steps to improve access to quality care by expanding our mental health care network to more than 300,000 providers, providing new ways for people to access care though telehealth and digital platforms, and using clinician-developed evidence-based guidelines to make coverage determinations.”
Lisa said she took on thousands in personal loans to pay for his treatment. She begged for help from New Mexico lawmakers. She told her story to the local newspaper, hoping to publicly shame the insurance company into providing her son the care he needed.
When UnitedHealthcare was persuaded to pay for a treatment center, the three in Albuquerque that accepted Medicaid rejected her son, calling his symptoms too complex. Out of pocket, such full-time residential treatment centers can cost more than $250,000 a year. Lisa found a private facility near Albuquerque called Villa Santa Maria willing to charge $500 a day. But UnitedHealthcare said it was willing to pay only $243, said Joe McGuill, who ran Villa Santa Maria.
McGuill said he vividly recalls the case because of how relentlessly the insurance company fought paying for treatment.
“Their number one thing was to deny, deny, deny,” he said. “They wanted me to turn down the mother and son, not admit him.”
McGuill said insurance officials tried to convince him that Lisa was too difficult to deal with and threatened to withhold future referrals from Villa Santa Maria. McGuill received unsolicited calls from hospitals and other providers that had previously treated the 10-year-old, telling him not to take the case.
Meanwhile, Lisa said the insurance company told her the closest option it would cover was a facility in Texas, nearly 600 miles away.
Knowing her son needed help, Lisa took him there. But she was so alarmed by the conditions that she asked state authorities to inspect the facility. Less than three weeks later, she said, Texas Family and Protective Services reported that it found several other kids had been beating up her son in the absence of adult supervision, including an incident in which a boy held a dining utensil to her son’s throat.
In a phone interview with The Post, her son described the trauma he experienced there. “I have this one memory of being put in a choke hold by another kid and facility staff just standing there, 10 feet away, watching me get hurt,” he said. “I remember staff threatening to cut up all my belongings in front of me, including a stuffed octopus that my sister gave me. I was alone, away from family, and that was my one symbol of home.”
The fifth-grader came out of the facility with a new diagnosis — post-traumatic stress disorder — and a deep hostility toward anyone claiming they wanted to help.
“It’s like the whole system decided to just flush this human being down the drain,” said his older sister, who watched as her brother cycled through one treatment program after another. “The insurance companies and Medicaid spent so much time fighting over where to send him and for how much. Now he doesn’t trust anyone, and it makes it that much harder for anyone to reach him.”
In 2015, a New Mexico newspaper ran a story on their struggle. A few days later, UnitedHealthcare finally agreed to fully cover her son’s care at Villa Santa Maria.
In a written statement, UnitedHealthcare confirmed that it authorized treatment for him at Villa Santa Maria.
Even then, McGuill said, “Every single month we’d have to defend him being there, because insurance wanted him out.”
The boy stayed at Villa Santa Maria for nearly a year. His suicidal impulses receded, and his emotions began to stabilize.
“Every single month we’d have to defend him being there, because insurance wanted him out.” — Joe McGuill, director of Villa Santa Maria
But to accomplish that, the staffers were physically restraining him as often as 40 times a month, holding down his hands and feet whenever he had an outburst until his rage subsided. The facility doesn’t dispute restraining him. Lisa knew why they were doing it but wrestled with the impact on her son and eventually pulled him out.
Like her son, Lisa had struggled with mental health, overcoming an eating disorder as a teen and severe depression as an adult.
“Now it’s my turn to teach [him],” Lisa wrote in her journal at the time. “To save him from himself. To help him find some reason to trust others even if it’s just me.”

‘He could kill her’
But as her son got older, his symptoms grew worse.
At 15, after overdosing on stolen prescription pills, he spat on nurses in the ER. He threatened to “shoot up at church,” according to hospital records. He vowed to the ER doctor trying to help him: “I’m going to find your name, find you in the street and cut your head off.” He expressed admiration for the Unabomber and copied lines from his manifesto onto his lunchbox.
By then, the family had moved to North Carolina, and Lisa’s marriage was crumbling. They divorced after her husband confessed to a social worker that he had molested their older daughter when she was a child, leading to criminal charges and a prison sentence. The revelations multiplied her son’s rage. He began ranting about the need to find and kill all pedophiles and liars.
Their house in North Carolina soon bore scars of his anger. Patched-up holes in the drywall. A broken water dispenser from when he picked up the five-gallon blue jug and threw it across the room. Cracks on his bedroom door after police had to kick it down.


Lisa bought plastic lockboxes and stowed away every sharp object in their home: scissors, knives, even tweezers. When he burned the lockboxes to force them open, she replaced them with heavy-duty metal safes.
Her younger sister, a retired police officer, got so worried for Lisa’s safety that she called the local sheriff’s department, begging them to arrest her nephew.
“I told them he could kill her. That he’s threatened to do it before,” said her sister Kelly Rowe Simpson, 57. But the authorities told her the boy was a minor and mentally ill. “They said they were already doing the maximum possible.”
Lisa’s life soon narrowed down to one wish — for her and her son to make it intact to his 18th birthday. She was already thinking about how to help him move out and establish his own life as an adult. He loved the outdoors and talked repeatedly of hiking the entire length of the Appalachian trail or driving across the country in a camper van.
For years, she wasn’t able to keep a full-time job because of his breakdowns. She dreamed of moving to Florida once he turned 18 and working full time again.
But those plans were upended at the end of January when he erupted again, threatening to hurt her. As Lisa secretly dialed 911 and edged her way to the front door, she realized they would never make it to his 18th birthday on their own.
For years, her son has denied his mental illness and substance use problems, often blaming his meltdowns on other people. But in an interview, the 17-year-old quietly acknowledged he has wrestled his whole life with a rage he can’t always control.
“Sometimes, when it gets really bad, I can actually feel it physically in my chest. It’s so uncomfortable that I’d do anything to stop it. I lash out. I’ve been aggressive. I’ve done things in the past that,” the teen paused, “yeah, that I regret.”
The years he spent being passed from one short-term treatment program to another only made everything worse, he said.
“These places, the whole system, I don’t feel like they’ve helped me,” he said.
Aside from Villa Santa Maria, which he praised, the facilities were almost always understaffed. The orderlies read from a script, he said, rather than treating children with real empathy. “The labels they put on you — oppositional disorder, Asperger’s — it’s like an excuse for them to dismiss you as a person, as worthless, as a problem. They don’t talk to you or try to find out what’s wrong. They just look at your chart. That’s all you are is a chart to them.”
When asked about his mom’s last-ditch effort to get him mental help by giving up custody, the teenager grew silent and then said, “I think it’s unfair that she has to do that.”
A crisis ignored
After drinking an entire bottle of gin in 2019, Lisa Rowe's son was rushed to the hospital with a nearly lethal blood alcohol level of 0.5 percent. He spent four days in a coma. (Family photo)")
There’s a term for mothers and fathers so desperate to get mental help for their children that they give up their parental rights — custody relinquishment.
The problem is at once widespread and utterly ignored. In 2003, the General Accountability Office issued a scathing report on the phenomenon. At least 12,000 families a year, it found, were forced to choose between keeping their children or getting them mental treatment. But the true number was probably many times more, because only 19 states kept track of such situations.
For the next two decades, the federal government’s response was to do nothing about the issue, even as rates of adolescent depression, mental illness and suicidal ideation skyrocketed. And as the cost of mental health treatment soared.
On the morning Lisa was scheduled to appear in court to relinquish custody of her son, a call woke her up in the middle of the night.
On the phone at 1:15 a.m. was a sheriff’s deputy telling her something had gone terribly wrong at the foster home where her son had been temporarily assigned by social workers.
“We found your son completely blacked out,” the deputy said. “He’s not responsive. We took him by ambulance to Pardee Hospital. He had a lot to drink. A lot.”
The way the deputy kept repeating “a lot” felt like an accusation: Where were you? Why weren’t you watching him?
Within minutes, Lisa was at the hospital’s front desk as she had been so many times before, trying to find her son.
Lying in the emergency room, his face was covered in scrapes and cuts from falling down.
“Oh, buddy,” she whispered to him, crying. “It’s going to be okay. I love you.”
Her son shivered. His eyes were open but staring into space. Doctors had put him in a neck brace and surrounded his hypothermic body in a plastic blanket inflated with warm air.
She’d spoken to her son just hours earlier. On the phone, he told her how he had gone out for Thai food with the foster family. After they hung up, authorities told Lisa, he’d apparently found three bottles of liquor in the foster family’s home and sneaked out. They found him unconscious and freezing on the street.
Lisa wondered, with guilt, if he’d been trying to return to her house. But soon, she was being led out of the room.
The hospital had gotten a call from social services. Because Lisa was in the process of relinquishing custody, she was no longer considered family and could not stay in her son’s room, hospital officials said. The government had been granted temporary guardianship.
Lisa furiously dialed the social services offices, but it was the middle of the night. No one answered.
She begged nurses in the waiting room for updates, but they said they were no longer allowed to tell her anything. So she sat in the hospital lobby, hoping to catch a glimpse if they transferred her son to another ward. She finally gave up at 4:30 a.m.
She didn’t want to be late for court.
Lisa Rowe drives home. Pending a court hearing, her son remains in temporary custody of social services. (Matt McClain/The Washington Post)")
Turning away
Her sister called as she began driving downtown toward the towering gray courthouse. Lisa was still fuming over being kicked out of her son’s room.
“This is the same hospital that was begging me just a few days ago to take him home, and now I can’t even see him,” she said. “All I wanted was to make sure he knew I was there.”
“Stop and breathe, Lisa,” her sister said. “They’re just doing their job. You can’t release custody of him and still demand to be there and involved in every decision. You can’t have it both ways. If you’re going to be mad at anyone, it’s him.”
She was mad at her son, she said. But she was mad at his mental illness, too. At society. And at herself.
“I really believe the reason he hurts me is that I’m his person in this world. The one person he can express what he’s feeling to,” she said. “What happens if I’m not there?”
She was still waiting for the family court judge to call her name two hours later, when a woman introduced herself as her court-appointed attorney.
“You don’t have to be here,” the lawyer said. “You’re not contesting them taking custody, right? I can enter it for you.”
“No,” Lisa insisted. “I want the judge to know I’m here.”
She wanted to explain why she was relinquishing her son, the rage he struggled with and what the government could do to help.
But she never got the chance. The hearing was over in a matter of seconds.
She stood when the judge called her name. Her lawyer spoke, “Your honor, my client would like it to be acknowledged that she’s here today.”
“Thank you, ma’am,” the judge said curtly before setting a date in seven weeks to revisit the matter in a fuller hearing. There would be no resolution of her son’s fate — and her own — until then.
Lisa walked back to her car in a daze.
“I love him. I miss him,” she said, shaking her head. “But the thought of living alone with him again, unable to keep him safe, to keep myself safe … I have to draw the line somewhere. I’m allowed to have a line, aren’t I?”
Her son’s case worker called to say that the hospital would be discharging him soon.
“I have to draw the line somewhere.” — Lisa Rowe
In her purse, Lisa Rowe keeps a stone with the word "Trust"” A hospital chaplain gave it to her while her son was in the ICU. She often runs her fingers across the engraved word as a reminder to trust that she and her son will somehow make it through their difficulties. (William Wan/The Washington Post)")
The good news: Now that he was the state’s responsibility, social services had accomplished something Lisa could not — convince a psychiatric facility to immediately admit her son. The bad news: The facility would keep him for only 30 days. It was unclear what would happen afterward.
“If he asks or anything,” said Lisa, uncertain when she would be allowed to speak to her son again, “be sure to tell him I love him.”
It was dark by the time she started the long drive home. She was at an intersection less than a mile from her house when she spotted a swarm of police cruisers on the road ahead, their blue and red lights piercing the night sky.
She wondered immediately if it was her son on the run again — this time from social services — trying to make his way home. What if he was hurt?
“I hope it’s not him,” she whispered, as her car idled at the red light.
She wanted to drive over just to make sure it wasn’t.
Instead, when the light flashed green, she turned right and headed home, alone.
Alice Crites contributed to this report.
About this story:
Story editing by Lynda Robinson. Photo editing by Mark Miller. Copy editing by Susan Doyle. Design by J.C. Reed.
[This article was originally published by The Washington Post.]