
Unscreened and Overlooked: Indian American Women Face Breast Cancer Risk
The story was co-published with India Currents as part of the 2025 Ethnic Media Collaborative, Healing California.


According to the American Cancer Society (2024) breast cancer rates are on the rise among Asian American women under the age of 50 in the United States.
The Cancer Nobody Warned Her About
It was early in the pandemic when Srila first noticed a lump in her breast.
“While showering, I used to feel a little bit of something tough, and it was like I felt it, but I did not pay much attention.”
Srila, a Bay Area health care professional, has spent over 20 years living in the U.S. and raising her family there. Though under five feet, she jokes that her energy and drive make her appear six feet tall on Zoom.
She was on track to have her biennial mammogram in 2020, but when the world shut down, and daily anxieties set in, she couldn’t focus on something that didn’t seem urgent. Srila had fundraisers to run for the Bay Area nonprofit she had co-founded to send critical pandemic supplies to India.
“I'm normally a very attentive and very science-driven person, but I think there was so much of that chaos with the pandemic going on,” she said.
But by August 2020, Srila could no longer ignore the grape-sized lump and tight, nagging sensation in her breast. When she called, her primary care physician insisted she come in immediately. She was 47.
The Rise of Breast Cancer in Young Asian Women Living in America
Srila had no way of knowing that breast cancer rates are on the rise among Asian American women under the age of 50 in the United States. According to a 2024 report from the American Cancer Society, AAPI women had the fastest-growing breast cancer incidence of any racial or ethnic group between 2012 and 2021, rising 2.6% per year.

Lihua Liu, PhD
Cancer was once considered a disease of the elderly, says Dr. Lihua Liu, a professor at the University of Southern California whose research explores differences in cancer risk by race and ethnicity and socioeconomic status, but the numbers say otherwise. Between 2000 and 2021, new breast cancer cases among AAPI women under 50 surged by 52%.
Additionally, a 2019 CDC study found that immigrant Asian women faced two to three times higher risk of developing breast cancer than their U.S.-born counterparts — even after accounting for known risk factors like reproductive history, BMI, and family history. This suggests something is elevating risk among women arriving from Asia, but the reasons why are still murky.
A Distinct Lack of Disaggregated Data
For Indian American women like Srila, this striking difference is even murkier as disaggregated data on South Asian communities is largely absent, making the true scope of their risk unknown.
Closer studies reveal important differences among these groups in screening rates, stage at diagnosis, treatment, and health outcomes. Census counts routinely lump together Asian Indian, Pakistani, Nepalese, Sri Lankan, and others, says Dr. Liu, making it nearly impossible to track breast cancer trends in specific South Asian populations.
Indian Americans are the second largest Asian group in the U.S. with a median age of 34. While there has been extensive media coverage about rising cancer rates among young people, far less attention has been paid to South Asians and their increasing risk of breast cancer. Heart disease and diabetes in South Asians receive far more attention, while cancer remains underemphasized.
“Science is always evolving, trying to find the answer, searching for the truth,” says Dr. Liu. “And then we realize ten, 20 years later — we thought we knew a lot already, but then later on, it was proven that we didn't know, or things can evolve.” Epidemiological research begins with surveillance, tracking patterns and trends at the population level, she explains. When patterns emerge, they serve as clues that prompt deeper investigation into the reasons behind them.

Dr. Preeti Farmah, MD, El Camino Health
Dr. Preeti Farmah, a breast surgical oncologist at El Camino Health in ountain View, California, says the risk factors for breast cancer are “either inherited or genetic, related to estrogen exposure, lifestyle, and environmental factors.”
For immigrant Asian American women, those lifestyle and environmental factors are increasingly shaped by the powerful force of westernization.
Westernization is a crucial risk factor for AAPI women
When Asian Americans move to the United States and adopt American lifestyles, the process of westernization has an important influence on breast cancer risk. Dr. Farmah explains that changes to diet, reproductive practices — like declines in fertility rate or having children later — and environmental exposures can make Asian American women more vulnerable.
Adopting a more westernized lifestyle results in higher rates of obesity, continued declines in the fertility rate, and a shift toward having children at a later age, according to Dr. Farmah. Early menarche — the onset of menstruation — and late menopause extend the body’s total window of estrogen exposure, modestly increasing breast cancer risk.
Like many Indian American women, Srila managed raising two children alongside her career, hobbies, volunteer work, and caring for her elderly in-laws.
Contending with career demands and working lifestyles in the U.S. also means that women tend to have fewer pregnancies and shorter breastfeeding duration, notes Dr. Farmah. “When women have fewer pregnancies, they go through menstrual cycles more frequently, and hence are more exposed to estrogen.” Chronic stress compounds this further, elevating cortisol levels in ways that may also increase risk.
Estrogen is food for cancer
As eating habits change, the food intake “involves higher fat diets with processed foods,” says Dr. Farmah. “There's a lot less physical activity as well.” Obesity compounds this risk further, Dr. Farmah adds, because “when you have fatty tissue, it can also produce estrogen.” She counsels her patients to think of estrogen as food — with greater estrogen exposure, cancer cells have more fuel to grow.
Dense breast tissue affects AAPI women at disproportionately high rates, though it's not clear why, says Dr. Farmah. This matters because both small breast cancers and dense tissue appear white on mammograms — fat looks dark, gray, or black — which makes them harder to detect. So often, says Dr. Farmah, the more subtle breast cancers remain unseen.
Having dense breast tissue also increases the likelihood of the tissue itself turning into cancer, adds Dr. Farmah, “because a lot of our cancer comes from cells within our glands or within our ducts.”
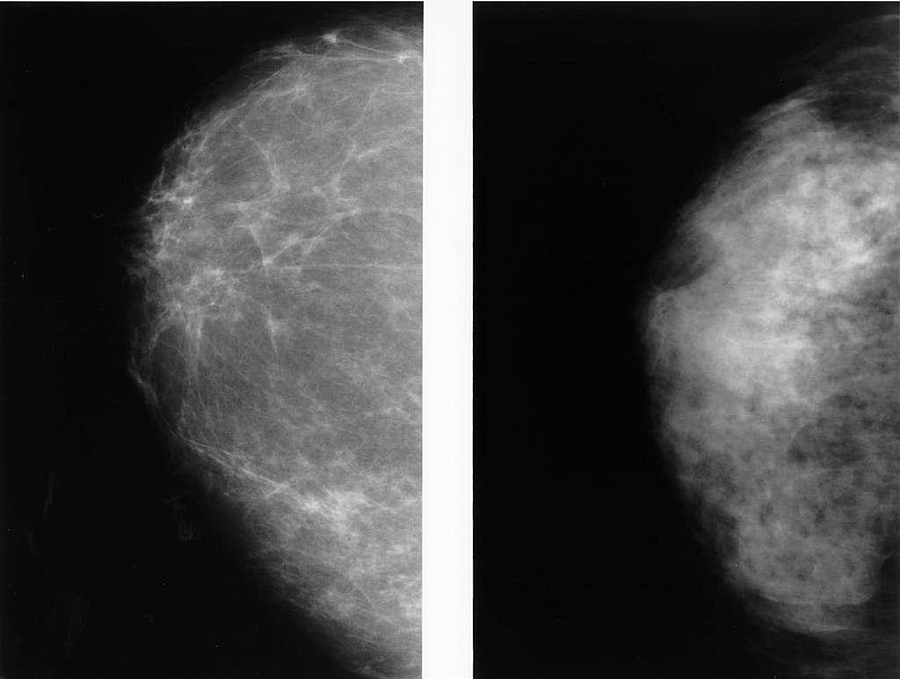
Abnormal lesions are easier to detect and diagnose in a fatty breast making mammography more accurate.
Dr. Kathy Cho. NIH Radiology // picryl.com
Cultural Barriers to Preventive Care
When first-generation Asian Americans delay getting preventive care, it's often because of cultural norms in health care behavior in their home countries that strongly influence how immigrants participate in their health care.
Patients may only visit doctors when they are actively sick, says Dr. Harpreet Pannu, a Kaiser internist in San Jose, who practiced medicine in India earlier in his career. Going to preventive care is not a habit, he explained, They often carry this mindset here.
Given that two thirds of Indian Americans were born outside the U.S., these cultural norms around preventive care are likely playing a critical role in how Indian American women approach getting mammograms.
“I think a lot of people just kind of think that oh, if I don't necessarily have a lump or any skin changes, I may not necessarily have a higher risk of breast cancer, and so I don't necessarily need to start my routine screening,” Dr. Farmah said.
In a Rutgers study of Indian and Pakistani women living in the U.S., researchers linked poor mammogram screening rates to lifestyle and cultural factors such as the lack of family support, lack of transportation, modesty around showing their breasts, and the belief that cancer is divine punishment for past deeds. Living in the United States for less than 10 years, low English proficiency, and a lack of confidence in the health system also contribute to low screening rates.
According to the CDC, AAPI women (aged 40 to 49) have among the lowest mammography rates of any racial group — only 54% reported a mammogram in the past two years, compared to 60% of White women.
As immigrant women adapt to a new culture, balance work and family, and navigate a new health care system, getting preventative care is often their last thought.
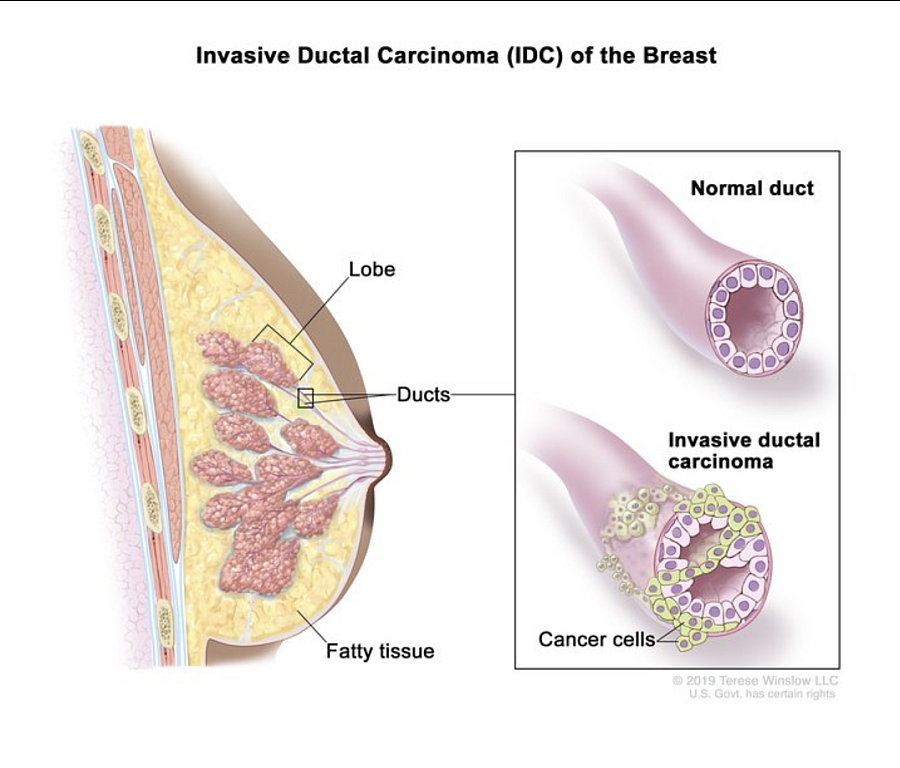
Anatomy of the female breast during invasive ductal carcinoma development.
National Cancer Institute
Benefits of Preventive Screening
Early detection pays off when immigrant women participate in health care screening programs.
Los Angeles resident Nibedita had her first mammogram when she turned 40 — the result was negative. Yet, a few months later, she felt a lump during a self-exam.
“I think I was sewing and just like, you know how you feel your body, right, and I felt something, and then I got more aware of it, and I self-checked.”
Her doctor sent her immediately for an ultrasound and biopsy, marking the beginning of her breast cancer journey.
The diagnosis was triple-negative breast cancer (TNBC), an aggressive form of the disease that, while relatively rare among AAPI women overall, occurs at higher rates in women of Indian subcontinent ancestry than in White women.
But caught early in a stage 1 diagnosis, Nibedita underwent a lumpectomy, chemotherapy, and radiation. She has been healthy since 2015, but recovery was painstakingly slow. “It took me almost, like five, six years to get back to that normal,” she says.
A Second Opinion and a Change of Plan
Things moved fast for Srila after her initial consultation. Within days, an ultrasound and a needle biopsy confirmed a triple-positive breast cancer diagnosis, which, she was reassured, “is the most curable one, so don't worry about it.”
After an initial recommendation for surgery before chemotherapy and radiation, Srila sent her test results to her sister, a physician in India, who advised a second opinion. This led Srila to an oncologist at Stanford who advocated chemotherapy first before surgery.
“He said your cancer is pretty big,” says Srila, “you have to reduce it first.”
Although the conflicting opinions were confusing, the Stanford physician ultimately convinced Srila. She started chemo at Stanford in October 2020 at the height of the pandemic, when restrictions meant her family could not help.
It was horrible. I had to do it alone.
Srila
The experience was debilitating — a high chemo dose for six to eight hours. The side effects were even worse: “severe diarrhea, like I can't even stand up from the sofa and go to the bathroom.” But she feels lucky that she could withstand the high dose of chemo.
After six cycles of chemo ended in January 2021, Srila’s surgery was scheduled in February. The cancer had reduced. “The doctor was happy that I was responding to that chemo regimen.”
The surgery, a lumpectomy, was successful, and in mid-April, she underwent radiation for two weeks every day. “May was my month of triumph,” says Srila.
But on June 5, Srila felt “fuzzy.” Something was not right. She was immediately admitted to the ER. The cancer had metastasized to her brain — there were 14 tumors.
Why the Cancer Wasn't Caught Earlier
In India, Srila’s anguished physician sister believed that Srila should have had a full-body PET scan after breast cancer treatment, a practice followed in the Indian health care system. Protocols in the U.S. recommend follow-up scans only if the patient starts showing symptoms. Her treatment plan at Stanford followed this protocol, and Srila confirmed.
Breast cancer chemo does not reach tumors in the brain, according to the Mayo Clinic, because the blood–brain barrier (BBB) blocks most large or potentially harmful molecules in the blood from entering the brain tissue. This makes treating brain tumors or metastases with chemotherapy much harder.
Srila underwent three sessions of a non-invasive, robotic radiation therapy system designed to precisely treat cancerous and benign tumors anywhere in the body.
Srila felt lucky. She was told that if she had 15 lesions, she would need full-brain radiation.
But the cancer kept coming back in 2022 and 2023. “It was already right inside the brain. So when you can see it, you will treat it, because it takes time to be visible,” said Srila.
In January 2024, Srila had a seizure. Doctors recommended immediate brain surgery. At the time, Srila was directing a musical and wanted to see it through. She begged her doctors for a respite. The day after the successful musical, she underwent surgery on the 12th of February: “They had to scoop it out completely along with any surrounding mass.”
Life has never been the same ever since.
Cognitive loss for sure. It took me a lot of rehab to climb up the stairs. Sometimes I couldn't feel that I had my left arm. I mean, it changed my life completely.
Srila
Srila is back to work and doing the things she enjoys like music and poetry, but – “everything is exhausting, and also it gives me dizziness.” Still under active treatment, Srila gets infusion treatment every 3 weeks and takes oral chemo medications daily. She undergoes a PET Scan, MRI, and echocardiogram every 2-3 months to track both the cancer and possible side effects to the heart.
Srila feels lucky to have received the specialized care she did, benefiting from cutting-edge technology and physicians who were deeply respectful of her needs.
“I don't want to live to breathe. I want to live to live. If I can't do my stuff, then I'm not living.”